7 results
Association of antibiotics with veteran visit satisfaction and antibiotic expectations for upper respiratory tract infections
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 23 June 2022, e100
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Long-term care facility employee infection prevention adherence and prevention of COVID-19 outbreaks in a high-incidence area
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s50-s51
-
- Article
-
- You have access
- Open access
- Export citation
-
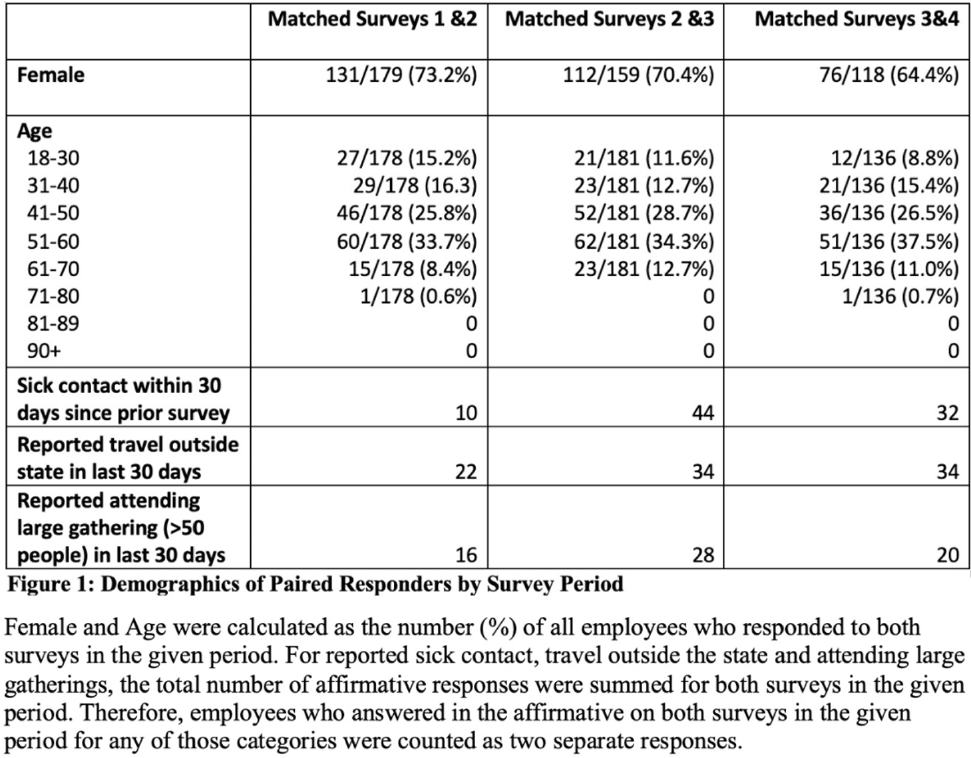
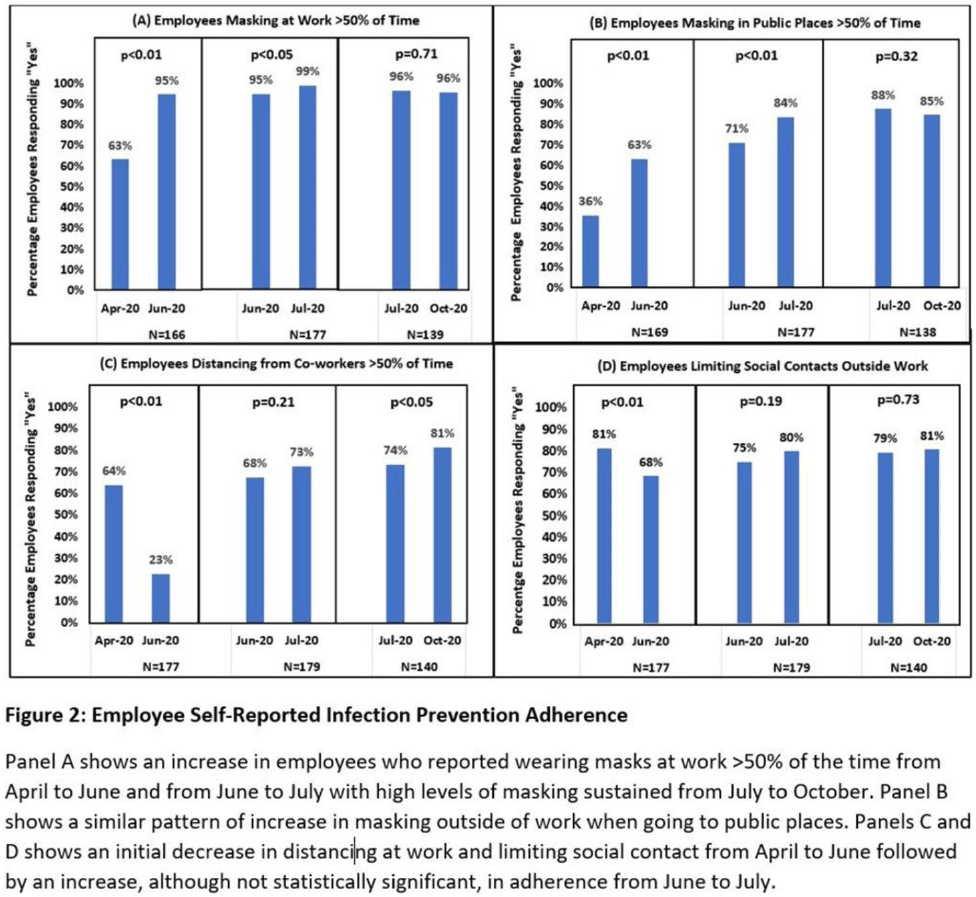
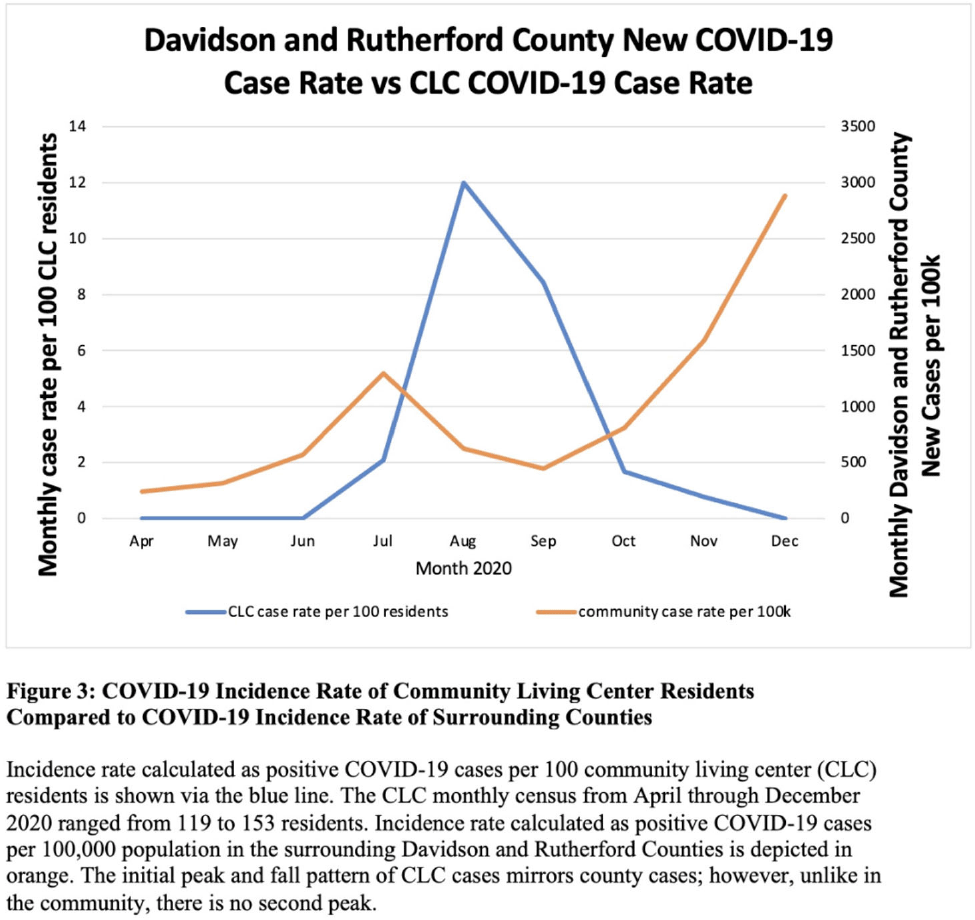
Background: Long-term care facility (LTCF) employees pose potential risk for COVID-19 outbreaks. Association between employee infection prevention (IP) adherence with facility COVID-19 outbreaks remains a knowledge gap. Methods: From April through December 2020, prior to COVID-19 vaccination, we tested asymptomatic Veterans’ Affairs (VA) community living center (CLC) residents twice weekly and employees monthly, which increased to weekly with known exposure, for SARS-CoV-2 via nasopharyngeal PCR. Employees voluntarily completed multiple choice questionnaires assessing self-reported IP adherence at and outside work. Surveys were longitudinally administered in April, June, July, and October 2020. Changes in paired employee responses for each period were analyzed using the McNemar test. We obtained COVID-19 community rates from surrounding Davidson and Rutherford counties from the Tennessee Department of Health public data set. CLC resident COVID-19 cases were obtained from VA IP data. Incidence rate and number of positive tests were calculated. Results: Between April and December 2020, 444 employees completed at least 1 survey; 177 completed surveys in both April and June, 179 completed surveys in both June and July, and 140 completed surveys in both July and October (Fig. 1). Across periods, employee surveys demonstrated an increase in masking at work and outside work between April and June (63% to 95% [P < .01] and 36% to 63% [P < .01], respectively), and June to July (95% to 99% [P < .05] and 71% to 84% [P < .01], respectively) that were both maintained between July and October (Fig. 2). Distancing at work and limiting social contacts outside work significantly decreased from April to June but increased in subsequent periods, although not significantly. COVID-19 community incidence peaked in July and again in December, but CLC resident COVID-19 cases peaked in August, declined, and remained low through December (Fig. 3). Discussion: Wearing a mask at work, which was mandatory, increased, and voluntary employee masking outside work also increased. CLC COVID-19 cases mirrored community increases in July and August; however, community cases increased again later in 2020 while CLC cases remained low. Employees reporting distancing at work and limiting social contacts outside work decreased preceding the initial rise in CLC cases but increased and remained high after July. Conclusions: These data from the pre–COVID-19 vaccination era suggest that widespread, increased support for and emphasis on LTCF IP adherence, especially masking, may have effectively prevented COVID-19 outbreaks in the vulnerable LTCF population.
Funding: None
Disclosures: None



259 Proton pump inhibitor use is not significantly associated with severe COVID-19 related outcomes after extensive covariate adjustment
-
- Journal:
- Journal of Clinical and Translational Science / Volume 6 / Issue s1 / April 2022
- Published online by Cambridge University Press:
- 19 April 2022, p. 43
-
- Article
-
- You have access
- Open access
- Export citation
Veteran Satisfaction for Upper Respiratory-Tract Infection (URI) Visits Is Not Associated with Antibiotic Receipt But Is Associated with Antibiotic Expectation
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s33
-
- Article
-
- You have access
- Open access
- Export citation
-
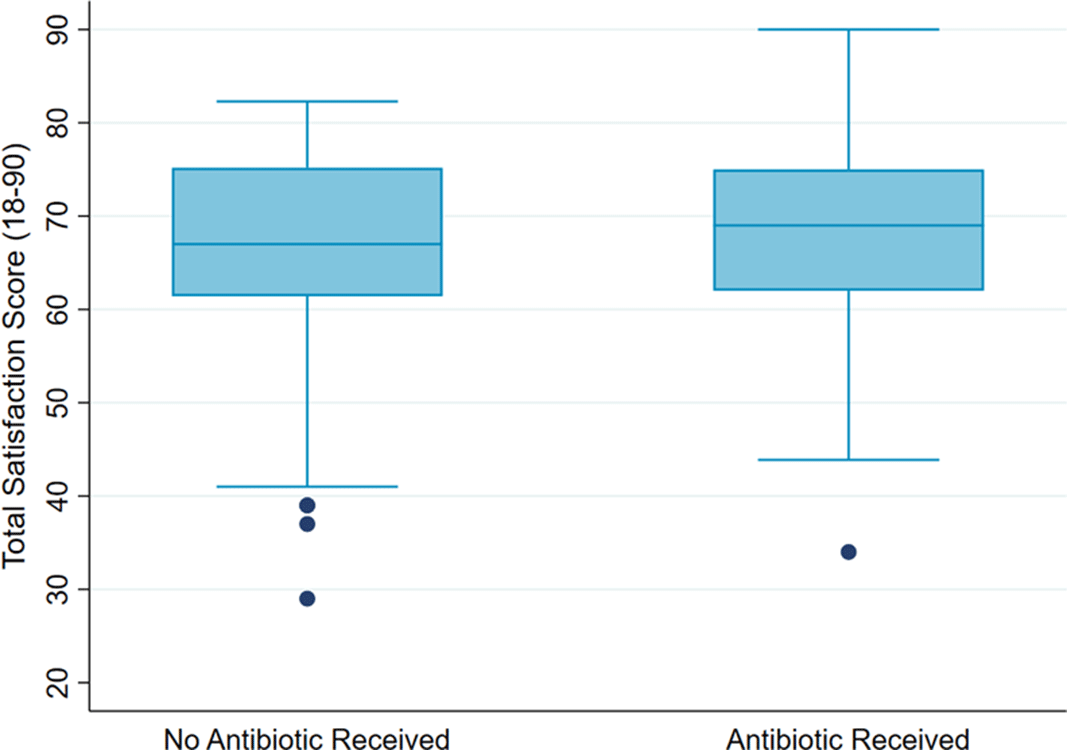
Background: Antibiotics are not recommended but are often prescribed for upper respiratory-tract infections (URIs). Prescribers cite patient expectation as a driver of inappropriate antibiotic prescribing; prior literature has demonstrated higher satisfaction scores in patients who receive antibiotics compared to those who do not. We assessed whether veteran satisfaction at URI visits was associated with antibiotic receipt or with reported expectation for antibiotics. Methods: We surveyed veterans with documented URI encounters in the Veterans’ Affairs Tennessee Valley Healthcare System between January 1, 2018, and December 31, 2019. Patients not evaluated in person, with documented dementia, or who died prior to the study start date were excluded. Veterans were asked to recall their URI visit and to complete the Patient Safety Questionnaire (PSQ)-18 (Rand Corporation) and questions assessing antibiotic expectations. The PSQ-18, an 18-item survey that assesses patient satisfaction, uses a 5-point Likert scale (ie, strongly disagree, disagree, uncertain, agree, strongly agree), yielding a composite score of 18–90. Higher scores represent more satisfaction with care. Demographic and visit-specific information were extracted via chart review. We used multivariable linear regression to assess differences in composite PSQ-18 satisfaction scores between those who did and did not receive an antibiotic, adjusted for patient and visit characteristics, and to assess differences in satisfaction scores for those who did and did not report expecting antibiotics, adjusted for antibiotic receipt. Results: We identified 1,435 patients seen for URI at 17 sites. After exclusions, 1,343 veterans were eligible for chart abstraction. After excluding 42 responders who responded after study close or returned blank surveys, the final analytic cohort included 432 (32.2%) of 1,343 responders; 225 (52.1%) received an antibiotic and 207 (47.9%) did not. Mean total satisfaction for veterans who received an antibiotic was 67.8 (SD, ±9.4) compared to 66.7 (SD, ±9.7) for those who did not (Figure 1). Increased total satisfaction was not significantly associated with antibiotic receipt (0.65; 95% CI, −2.0 to 3.3). Most veterans (72.0%) disagreed that visit satisfaction depended on antibiotic receipt. However, only 30.8% reported that they would not expect an antibiotic for URI visits. A significant reduction in total satisfaction (−4.1; 95% CI, −6.3 to −1.9) was associated with expecting compared to not expecting an antibiotic. Conclusions: Our findings suggest that prescribing an antibiotic is not associated with increased veteran satisfaction for URI visits but is associated with expecting an antibiotic. Future work will evaluate methods to change veteran antibiotic expectations.
Funding: No
Disclosures: None
Figure 1.

Use of the brief Confusion Assessment Method in a veteran palliative care population: A pilot validation study
-
- Journal:
- Palliative & Supportive Care / Volume 17 / Issue 5 / October 2019
- Published online by Cambridge University Press:
- 19 March 2019, pp. 569-573
-
- Article
- Export citation
2506 Post-discharge opioid prescriptions and their association with healthcare utilization in the Vanderbilt Inpatient Cohort Study
-
- Journal:
- Journal of Clinical and Translational Science / Volume 2 / Issue S1 / June 2018
- Published online by Cambridge University Press:
- 21 November 2018, p. 86
-
- Article
-
- You have access
- Open access
- Export citation
2156: A confounder assessment of patient frailty in the relationship between antidiabetic medication and heart failure
-
- Journal:
- Journal of Clinical and Translational Science / Volume 1 / Issue S1 / September 2017
- Published online by Cambridge University Press:
- 10 May 2018, pp. 24-25
-
- Article
-
- You have access
- Open access
- Export citation