6 results
Multicenter evaluation of contamination of the healthcare environment near patients with Candida auris skin colonization – ERRATUM
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 07 October 2022, e166
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Outbreak investigation of CRAB at an acute-care hospital ICU during the COVID-19 pandemic–Chicago, Illinois, March 2020–September 2021
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s84
-
- Article
-
- You have access
- Open access
- Export citation
-
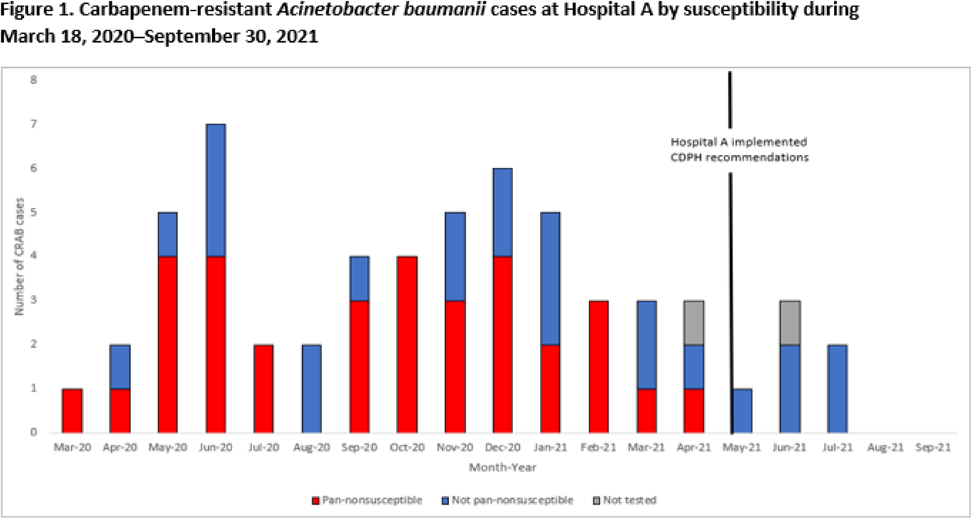
Background: Carbapenem-resistant Acinetobacter baumannii (CRAB) is primarily associated with hospital-acquired infections and is an urgent public health threat due to its ability to contaminate the environment and cause severe disease. In 2019, Illinois began pilot surveillance for CRAB requiring select laboratories to submit specimens for molecular characterization. On July 17, 2020, the Chicago Department of Public Health (CDPH) was notified of an increase in CRAB infections in a 20-bed ICU at an acute-care hospital in Chicago (hospital A) during the initial COVID-19 surge. We summarize the outbreak investigation findings and infection control recommendations. Methods: Clinical cultures were collected from patients in hospital A, and CRAB-positive isolates were sent to the Wisconsin State Laboratory of Hygiene for mechanism of resistance and antibiotic susceptibility testing. On-site assessments and remote follow-ups were conducted by CDPH infection preventionists to evaluate infection control practices including environmental cleaning, hand hygiene compliance, and use of personal protective equipment (PPE). The Illinois Department of Public Health and CDPH summarized the testing results, facilitated a containment response, and provided recommendations for infection control. Results: From March 18, 2020, to September 30, 2021, 56 patients with CRAB infections were identified from hospital A, and 33 (59%) of these cases were pan-nonsusceptible. Most specimen sources were sputum (n = 30, 54%), followed by blood (n = 13, 23%), urine (n = 6, 11%) and other (n = 7, 13%). Among isolates with mechanism testing (n = 54), 45 (83%) were positive for OXA-24/40 and 9 (17%) were positive for OXA-23. Of the CRAB-positive patients, 28 (50%) were previously positive for SARS-CoV-2. To date, 25 of these patients (45%) have been discharged and 31 (55%) have died. Two onsite visits and 7 remote-assistance sessions were conducted as part of the investigation. In response to increased COVID-19 hospitalizations, hospital A moved to crisis-capacity PPE use and encountered staffing shortages, which led to compromised infection control measures. Cleaning agents (Quat disinfectant cleaner) were also found to be ineffective against CRAB and required long contact times. Conclusions: In response to the CRAB outbreak at hospital A, CDPH recommended that the hospital stop crisis-capacity protocols for PPE, conduct admission screening and point-prevalence testing for CRAB, implement a hand hygiene campaign, and use an EPA-registered List K product for environmental cleaning. These recommendations were implemented in May 2021, and no CRAB cases have been reported since July 2021. To reduce CRAB transmission during the pandemic, facility leadership must commit resources to educate staff on effective infection control practices including conventional use of PPE, appropriate cleaning agents, and improved hand hygiene.
Funding: None
Disclosures: None

Multicenter evaluation of contamination of the healthcare environment near patients with Candida auris skin colonization
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s78-s79
-
- Article
-
- You have access
- Open access
- Export citation
-
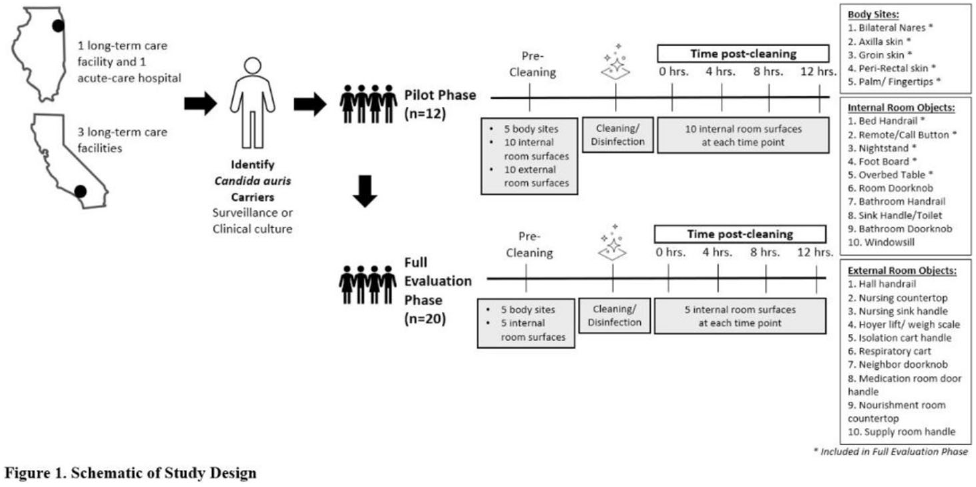
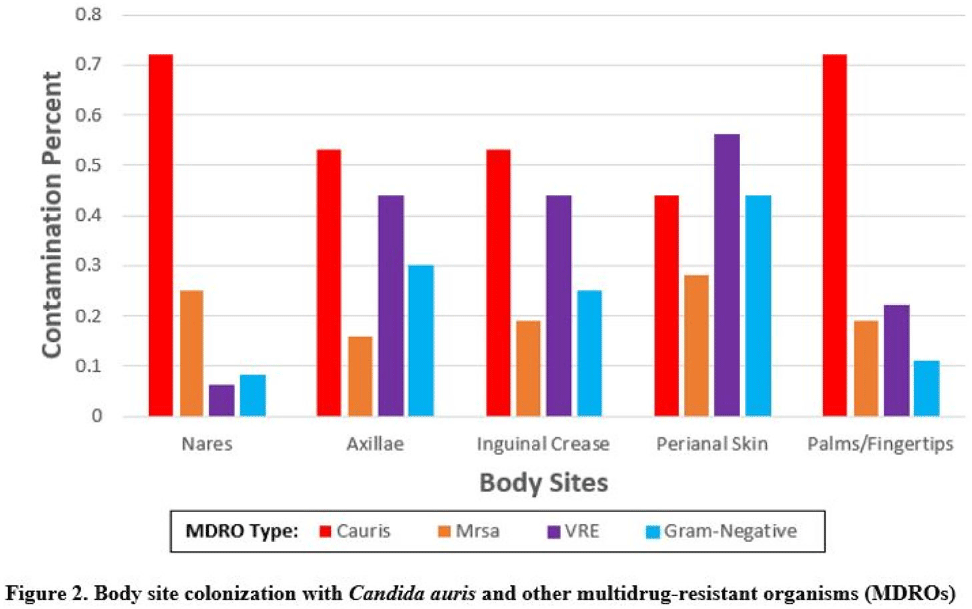
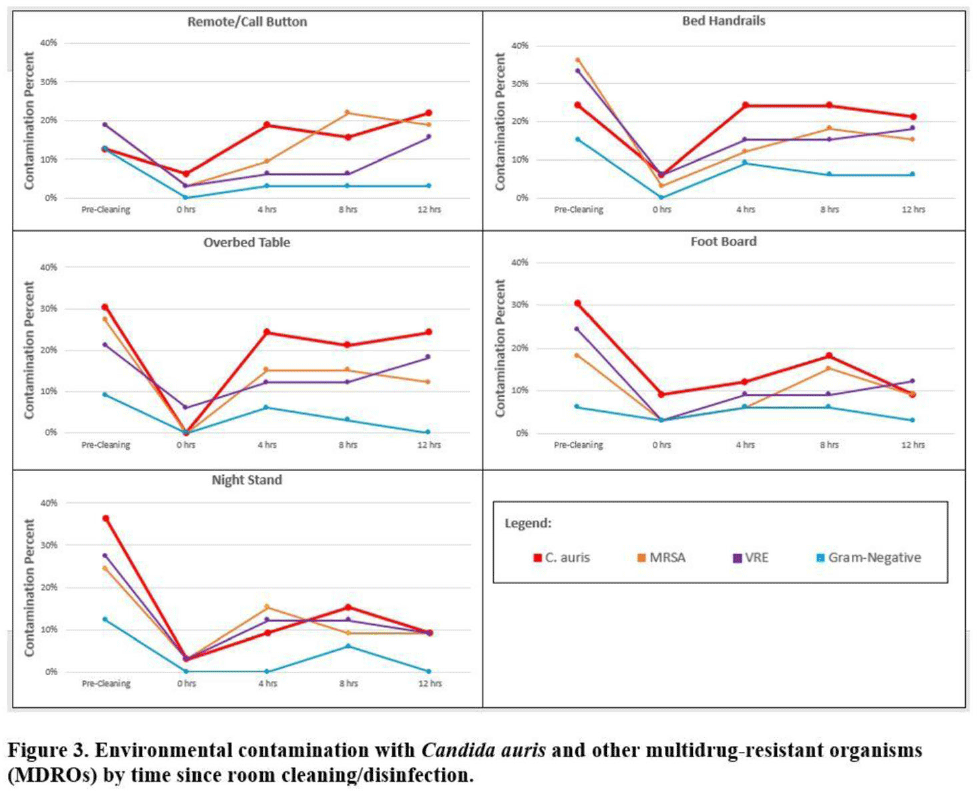
Background:Candida auris is an emerging multidrug-resistant yeast that is transmitted in healthcare facilities and is associated with substantial morbidity and mortality. Environmental contamination is suspected to play an important role in transmission but additional information is needed to inform environmental cleaning recommendations to prevent spread. Methods: We conducted a multiregional (Chicago, IL; Irvine, CA) prospective study of environmental contamination associated with C. auris colonization of patients and residents of 4 long-term care facilities and 1 acute-care hospital. Participants were identified by screening or clinical cultures. Samples were collected from participants’ body sites (eg, nares, axillae, inguinal creases, palms and fingertips, and perianal skin) and their environment before room cleaning. Daily room cleaning and disinfection by facility environmental service workers was followed by targeted cleaning of high-touch surfaces by research staff using hydrogen peroxide wipes (see EPA-approved product for C. auris, List P). Samples were collected immediately after cleaning from high-touch surfaces and repeated at 4-hour intervals up to 12 hours. A pilot phase (n = 12 patients) was conducted to identify the value of testing specific high-touch surfaces to assess environmental contamination. High-yield surfaces were included in the full evaluation phase (n = 20 patients) (Fig. 1). Samples were submitted for semiquantitative culture of C. auris and other multidrug-resistant organisms (MDROs) including methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus (VRE), extended-spectrum β-lactamase–producing Enterobacterales (ESBLs), and carbapenem-resistant Enterobacterales (CRE). Times to room surface contamination with C. auris and other MDROs after effective cleaning were analyzed. Results:Candida auris colonization was most frequently detected in the nares (72%) and palms and fingertips (72%). Cocolonization of body sites with other MDROs was common (Fig. 2). Surfaces located close to the patient were commonly recontaminated with C. auris by 4 hours after cleaning, including the overbed table (24%), bed handrail (24%), and TV remote or call button (19%). Environmental cocontamination was more common with resistant gram-positive organisms (MRSA and, VRE) than resistant gram-negative organisms (Fig. 3). C. auris was rarely detected on surfaces located outside a patient’s room (1 of 120 swabs; <1%). Conclusions: Environmental surfaces near C. auris–colonized patients were rapidly recontaminated after cleaning and disinfection. Cocolonization of skin and environment with other MDROs was common, with resistant gram-positive organisms predominating over gram-negative organisms on environmental surfaces. Limitations include lack of organism sequencing or typing to confirm environmental contamination was from the room resident. Rapid recontamination of environmental surfaces after manual cleaning and disinfection suggests that alternate mitigation strategies should be evaluated.
Funding: None
Disclosures: None



Regional Impact of a CRE Intervention Targeting High Risk Postacute Care Facilities (Chicago PROTECT)
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s48-s49
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Repeated Prevalence Surveys and Admission Screening for Candida auris at One Long-Term Acute-Care Hospital, Chicago, 2016–2019
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s14-s15
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Candida auris and Carbapenemase-Producing Organism Prevalence in an Extended Stay Pediatric Hospital, Chicago, Illinois, 2019
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s145-s146
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation