Contents
Poster Presentation - Poster Presentation
Antibiotic Stewardship
Racial and ethnic differences in penicillin allergy reporting and allergist referral
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s23
-
- Article
-
- You have access
- Open access
- Export citation
-
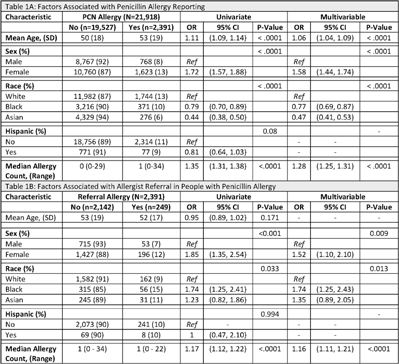
Background: Antimicrobial resistance (AMR) is a global public health crisis. A key strategy to combat AMR is to use targeted antibiotics, which is difficult in patients who report an allergy to penicillin. Increased risk for resistant infections, mortality, and healthcare costs are associated with penicillin allergies; however, up to 90% of those with a reported penicillin allergy do not have a true allergy. We investigated racial and ethnic differences related to penicillin allergy delabeling by analyzing rates of penicillin allergy reporting and referral for allergist consultation. Methods: Tufts Medical Center is a teaching medical center in Boston, Massachusetts. This study cohort contains all patients seen in 2019 by clinicians at Primary Care Boston, the main primary care practice at Tufts Medical Center. Demographic data, documented allergies, and referral history were collected from the electronic medical record. We performed univariate and multivariable analyses using logistic regression models. Covariates found to be statistically significant (P < .05) in the univariate analyses were included in the multivariable model. Results:In total, 2,391 (11%) patients reported a penicillin allergy, but only 249 (10%) were referred to an allergist (Table 1). Black patients and Asian patients were less likely to report a penicillin allergy than White patients. We detected no differences related to Hispanic ethnicity. Black patients with penicillin allergy were more likely to be referred to an allergist. Conclusions: There were low rates of allergist referral for penicillin allergy delabeling in this cohort. We identified racial differences in both penicillin allergy reporting and allergist referral. Allergist consultation is an important opportunity to combat AMR and should be considered for all patients reporting a penicillin allergy. Future work should evaluate equitable access to allergy delabeling resources.
Funding: None
Disclosures: None

Antimicrobial use patterns during the COVID-19 pandemic at an academic medical center
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s23-s24
-
- Article
-
- You have access
- Open access
- Export citation
-
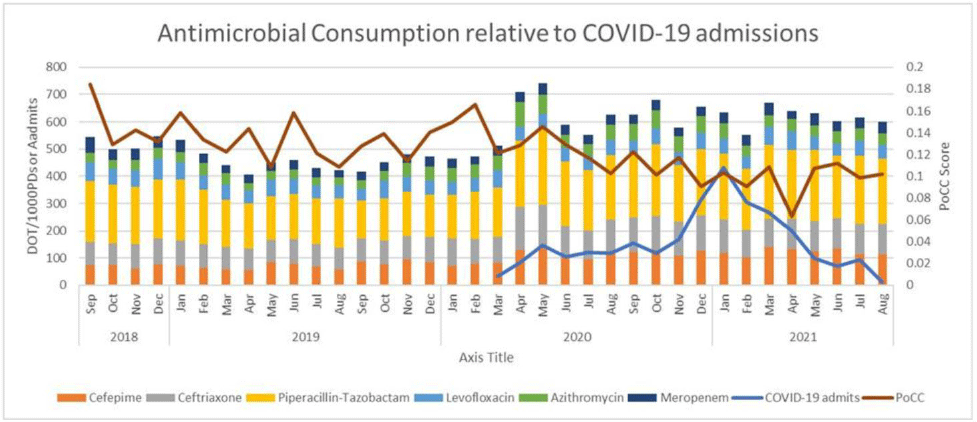
Background: The COVID-19 pandemic has made a significant impact on antimicrobial use patterns across health systems. We have described antibiotic use patterns at an academic medical center in Richmond, Virginia, before and after the onset of COVID-19. We also examined the impact on the proportional consumption of carbapenems (PoCC) metric. PoCC represents meropenem utilization relative to the narrower-spectrum antipseudomonal agents cefepime and piperacillin-tazobactam. Our institution practices antimicrobial restriction for meropenem. All other antibiotics included in the study data can be freely ordered by any provider. Methods: We evaluated antimicrobial use data from September 2018 through August 2021 using days of therapy (DOT) per 1,000 patient days. We included 18 months of data before and after the first recorded COVID-19 admission at our institution in March 2020. Mean comparisons were performed using the Welch 2-sample t test. The Bonferonni correction for multiple comparisons was utilized to determine significance with an initial baseline α of 0.05. All data analyses were performed using R software (R Foundation for Statistical Computing, Vienna, Austria, 2021). Results: Normality was evaluated with QQ-plots and all data demonstrated normality. Bonferroni correction produced an adjusted α value of 0.007. We detected significant increases in the use of cefepime, piperacillin-tazobactam, ceftriaxone, and azithromycin following the onset of the COVID-19 pandemic. We noted a significant decrease in the PoCC metric during this period. No significant change was noted for levofloxacin or meropenem. Conclusions: The COVID-19 pandemic produced significant changes in antimicrobial use patterns at our institution. We noted statistically significant increases in bacterial community-acquired pneumonia-focused antibiotics (ceftriaxone and azithromycin). We observed significant increases for cefepime and piperacillin-tazobactam. Interestingly, relative utilization of carbapenems as measured by the PoCC metric continued to decrease during this time. This trend was primarily driven by increases in cefepime and piperacillin-tazobactam utilization while meropenem utilization remained relatively constant. This study highlights the importance of looking at normalized antibiotic consumption data and not relative-use data alone.
Funding: None
Disclosures: None

Recommendations for antimicrobial stewardship during end-of-life patient care
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s24
-
- Article
-
- You have access
- Open access
- Export citation
Assessment of antibiotic appropriateness in hospitalized veterans with COVID-19 in the VA MidSouth Healthcare Network (VISN9)
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s24-s25
-
- Article
-
- You have access
- Open access
- Export citation
-
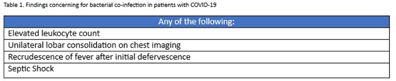
Background: Bacterial coinfections with COVID-19 appear to be rare, yet antibiotic use in this population is high. Limited guidance is available regarding the use of antibiotics in these patients. In response, a multidisciplinary group of physicians and pharmacists from 5 VISN9 facilities developed a guideline for the use of antibiotics with COVID-19 in July 2021. This guideline created a network-wide standard for antibiotic use and facilitates the assessment of antibiotic appropriateness in hospitalized veterans with COVID-19. Methods: In this observational, cross-sectional study, we reviewed veterans diagnosed with COVID-19 from August 1 through September 30, 2021, who were admitted to VISN9 facilities. Use of antibiotics was assessed during the first 4 days of admission. If antibiotics were prescribed, their use was determined to be appropriate or inappropriate based on the presence or absence of a finding concerning for bacterial coinfection as outlined in the guideline (Table 1). Additional data including procalcitonin results as well as positive sputum cultures were collected. Results: In total, 377 veterans were admitted for COVID-19 during the study period. Among them, 42 veterans (11%) received antibiotics for nonrespiratory infections and were removed from this analysis. Of the remaining 335 veterans, 229 (68%) received antibiotics and 116 (51%) of those met guideline criteria that were concerning for bacterial coinfection. Additionally, 32 (14%) of the 229 veterans who received antibiotics had >1 finding concerning for bacterial coinfection. Procalcitonin levels were obtained in 97 (42%) of 229. Only 33 veterans (14%) who received antibiotics had an elevated procalcitonin, and only 19 (8%) had a positive sputum culture. Conclusions: Antibiotic use was common in hospitalized veterans with COVID-19 in VISN9 facilities. This results are comparable to findings in the published literature. Among those receiving antibiotics early in their hospitalization, half were considered appropriate based on our guideline. Quality improvement initiatives are needed to improve implementation of the network guideline to reduce the overuse of antibiotics for management of COVID-19. Additionally, procalcitonin may be a helpful tool for hospitalized veterans with COVID-19.
Funding: None
Disclosures: None

Assessing the association between cefepime percentage free trough level and neurotoxicity
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s25
-
- Article
-
- You have access
- Open access
- Export citation
-
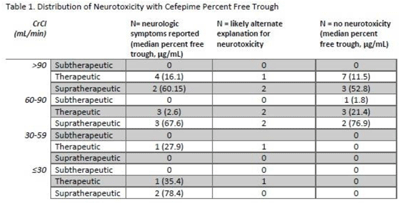
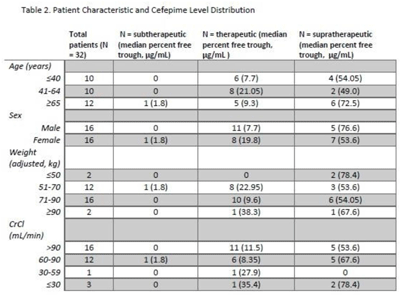
Background: Cefepime has a known association with neurotoxicity due to its ability to cross the blood–brain barrier. The symptoms of neurotoxicity are highly variable. It has been postulated that cefepime neurotoxicity is associated with elevated levels of the drug. However, studies assessing for an association between serum drug level and the incidence of neurotoxicity have yet to establish a consistent threshold. We assessed serum cefepime levels and incidence of neurotoxicity to help develop a dosing strategy to minimize adverse effects. Method: In total, 32 inpatients admitted from January 2019 to November 2021 who received cefepime according to institutional standard dosing regimens for at least 72 hours were reviewed by infectious diseases pharmacists who obtained serum cefepime levels and performed pharmacokinetic analyses to obtain percentage free trough levels. Cefepime percentage free trough levels were defined as therapeutic if they were above the known minimum inhibitory concentration (MIC) of the treated organism and were <40 μg/mL. Patient charts were reviewed for clinical findings consistent with cefepime-induced neurotoxicity. Numerical and statistical analyses were performed to assess factors with a significant association with neurotoxicity. Results: Overall, 16 (47.1%) patients showed some evidence of neurotoxicity, 9 (56.3%) of whom had a likely alternate clinical cause of symptoms (Table 1). We did observe that patients with creatinine clearance <60 mL/min were more likely to have symptoms concerning for neurotoxicity. Conclusions: Cefepime percentage free trough levels were highly variable, and no association with neurotoxicity was observed. Patients with decreased creatinine clearance were significantly more likely to develop neurologic findings consistent with cefepime-induced neurotoxicity. Further study is needed to establish a relationship between cefepime pharmacokinetic values and incidence of neurotoxicity.
Funding: None
Disclosures: None


Implementing Leading antimicrobial stewardship practices in United States hospitals – A qualitative study
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s25-s26
-
- Article
-
- You have access
- Open access
- Export citation
Systematic review of antibiotic stewardship interventions for urinary tract infection management in the ambulatory setting
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s26
-
- Article
-
- You have access
- Open access
- Export citation
Antibiotic use and impact on illness course in children with influenza-like-illness in the emergency department
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s26
-
- Article
-
- You have access
- Open access
- Export citation
C. difficile
In veteran outpatients, antibiotics remain significant risk factor for community-acquired Clostridiodes difficile infection
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s26-s27
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: An estimated 30% of antibiotic prescriptions in outpatient settings may be inappropriate. Antibiotic exposure increases an individual’s risk of Clostridioides difficile infection (CDI). To assess the prevalence of community-acquired CDI (CA-CDI) among patients without recent hospitalization and to examine the influence of outpatient antibiotic exposure on the risk of acquiring CA-CDI in this population, we examined a 2-year cohort of patients seen in primary care clinics at VA community-based outpatient clinics (CBOCs) associated with a large VA medical center. Methods: All primary care visits and nonvisit antibiotic prescriptions were identified in calendar years 2018–2019 as encounters of interest. Encounters occurring Results: We identified 84,787 patients with visits meeting our criteria. In this cohort, 3,533 patients were prescribed antibiotics at their encounter of whom 5 (0.14%) developed CA-CDI. Among the 81,254 patients who were not prescribed antibiotics, 15 (0.02%) developed CA-CDI, yielding an unadjusted CA-CDI odds ratio of 7.68 (95% CI, 2.50–19.82). p Conclusions: Although CA-CDI episodes were infrequent among VA outpatients with a CBOC visit in 2018–2019, the odds of CA-CDI were 7-fold greater in outpatients with antibiotic exposure than outpatients without antibiotic exposure. Antibiotic stewardship interventions that emphasize adverse events as a result of care provided in the outpatient setting, rather than as events limited to acute-care settings, may mitigate CDI risk.
Funding: This work was supported by the Merck Investigator Studies Program (MISP 59266 to F.P. and R.J.), and funds and facilities were provided by the Cleveland Geriatric Research Education and Clinical Center (GRECC) at the VA Northeast Ohio Healthcare System. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclosures:. All authors report no conflicts of interest relevant to this article. R.J. has received research funding from Pfizer; she has also participated in advisory boards for Pfizer and Merck.


Characteristics of antibiotic exposures for surgical procedures prior to Clostridioides difficile diagnosis—Minnesota, 2018
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s27
-
- Article
-
- You have access
- Open access
- Export citation
Clostridioides difficile: A diagnostic intervention
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s27
-
- Article
-
- You have access
- Open access
- Export citation
Clostridioides difficile infection (CDI) treatment outcomes and recurrence factor at a pediatric hospital
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s28
-
- Article
-
- You have access
- Open access
- Export citation
Role of diagnostic stewardship in reducing healthcare facility-onset Clostridioides difficile infections
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s28-s29
-
- Article
-
- You have access
- Open access
- Export citation
-
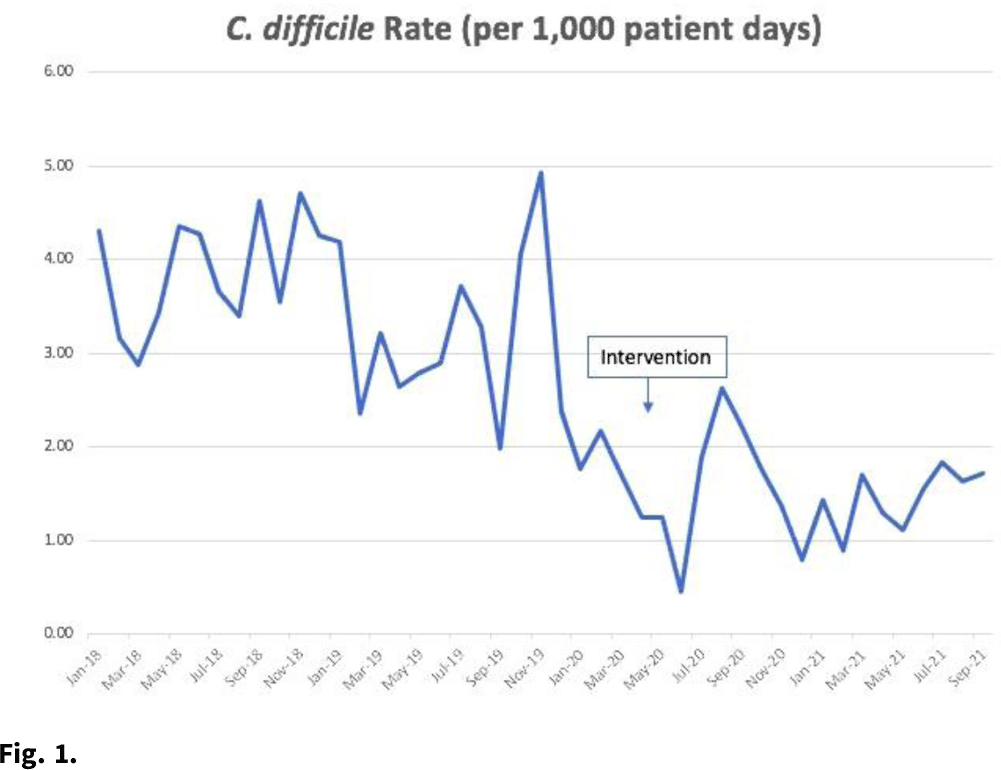
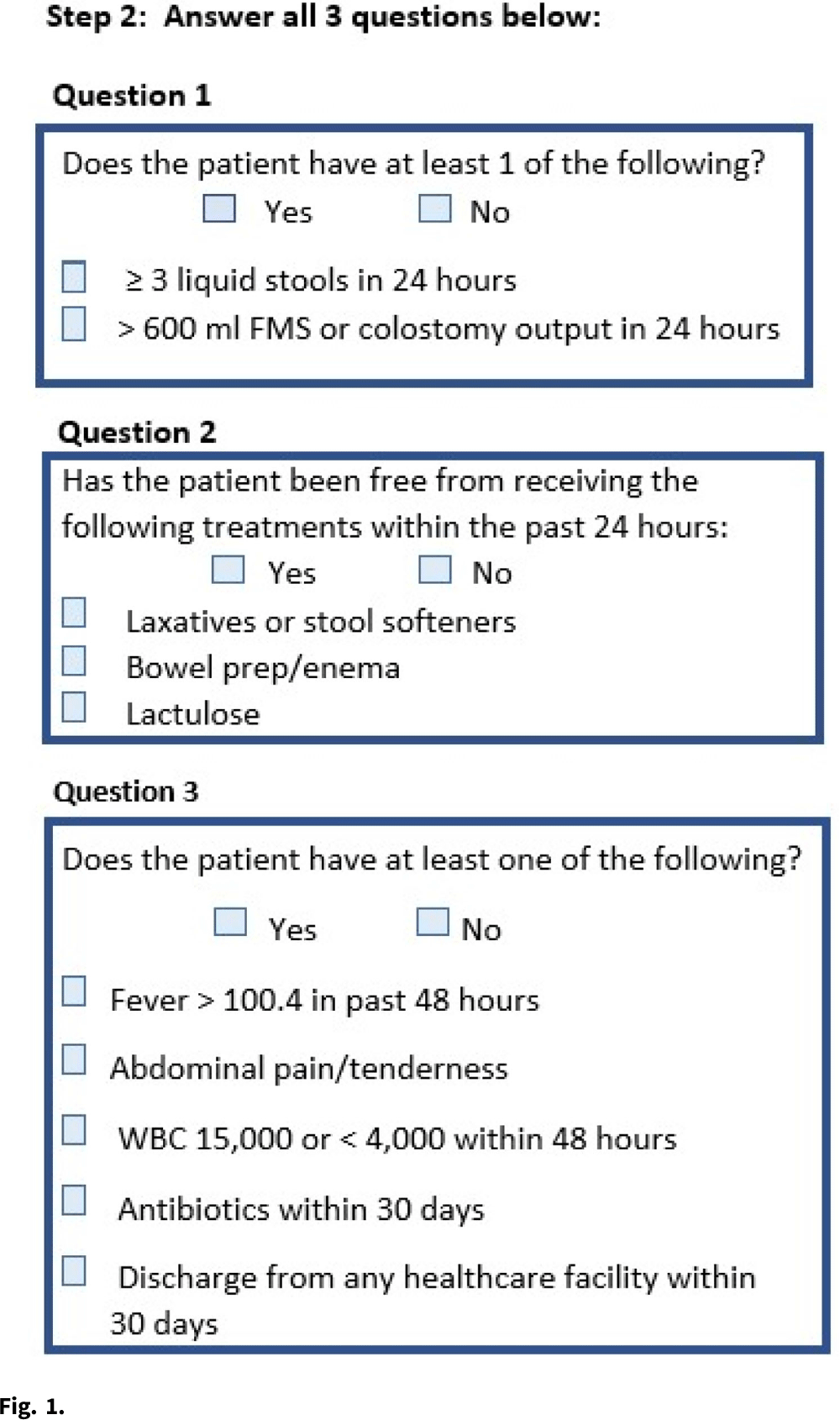
Background:Clostridioides difficile infection (CDI) is the most common healthcare-associated infection (HAI) in the United States. Healthcare facility-onset (HO) CDI reporting is a laboratory-identified (LabID) event and does not rely on symptoms. Inappropriate testing can lead to overdiagnosis in patients who are colonized, especially in those receiving promotility agents. Approximately 45% of HO-CDI cases at our institution occurred in the setting of laxative use in 2019. We assessed the effectiveness of an electronic medical record (EMR) “hard stop” in reducing inappropriate CDI testing and its impact on HO-CDI rates. Methods: We conducted a pre–post quasi-experimental retrospective study comparing test order rates per 1,000 patient days, CDI rate per 1,000 patient days, and standardized infection ratio (SIR) in the preintervention period (January 2018–December 2019) to the intervention period (April 2020–September 2021), at a 5-hospital healthcare system in southeastern Michigan. In February 2020, we implemented a hard stop in Epic that was triggered >3 days after admission for the following criteria: patients <1 year of age; repeated testing within 7 days, and receipt of promotility agents within 48 hours. After discontinuing the promotility agents for at least 48 hours, providers were allowed to place an order if diarrhea persisted. The medical director of infection prevention and control or designee had the ability to override the hard stop when deemed necessary after reviewing the case upon provider request. All orders expired after 24 hours if a specimen was not collected. We retrospectively reviewed the number of overrides after the intervention to determine the positivity rate. Results: Our CDI rates per 1,000 patient days were 3.21 in the preintervention period and 1.48 in the postintervention period, a 54% reduction (Fig. 1). The test order rates were 119.4 in the preintervention period and 87.7 in the postintervention period, a 26.5% reduction (Fig. 2). The SIR decreased from 0.542 in the preintervention period to 0.361 in the postintervention period, a 33% reduction (95% CI, 0.54–0.82; P = .0001). After the intervention, 299 patients had an override. Of these, samples from 218 patients (72.9%) were negative, 50 orders (16.7%) were cancelled, and 28 samples (9%) were positive. Conclusions: Diagnostic stewardship, utilizing an electronic hard stop, was effective in reducing inappropriate C. difficile testing in the setting of promotility agents without delaying diagnosis of HO-CDI. This strategy combined with standard best practices can significantly reduce HO-CDI rates.
Funding: None
Disclosures: None


Prospective audit and feedback of Clostridioides difficile PCR at the time of ordering increases appropriateness of testing
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s29
-
- Article
-
- You have access
- Open access
- Export citation
-
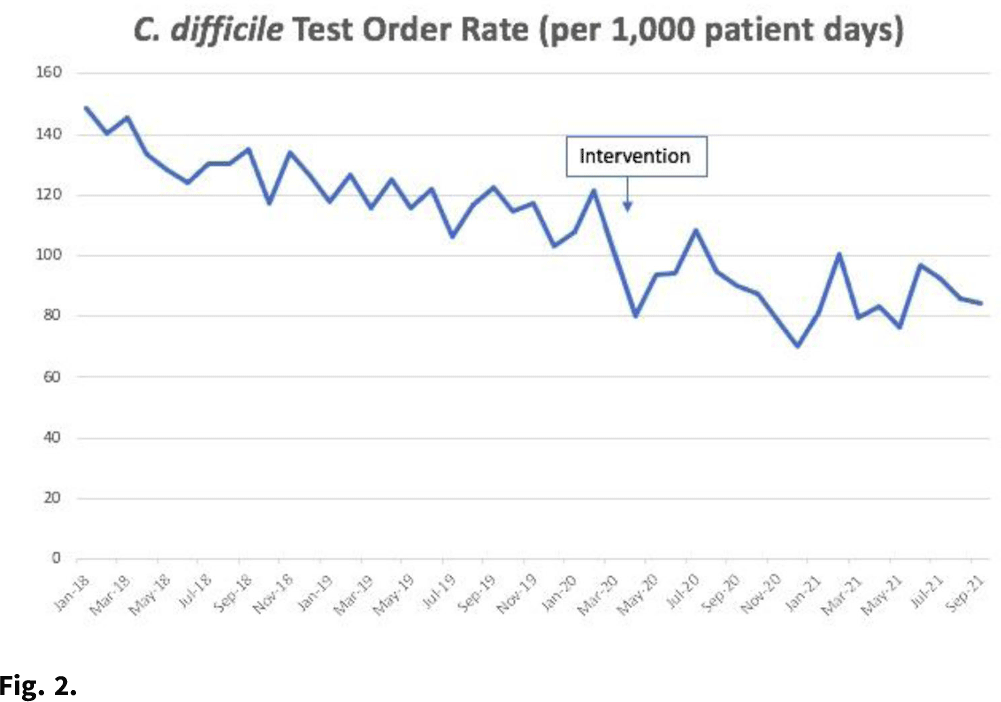
Background: Over-testing for Clostridioides difficile infection outside acute diarrheal illness without a clear alternative cause can lead to inappropriate diagnosis and treatment with antibiotic therapy. Preanalytical interventions such as education, order restriction, and electronic order assistance are common but are limited in effectiveness. As an alternative approach, our antibiotic stewardship program (ASP) implemented prospective audit and feedback (PAF) on C. difficile PCR orders to reduce inappropriate testing.
Methods: The study was conducted at a 399-bed, tertiary-care, Veterans’ Affairs Medical Center and included adult inpatients and outpatients for whom C. difficile PCR testing was ordered. In the preintervention period from June through September 2019, the ASP was alerted to C. difficile PCR tests and collected data but did not intervene. From October 2019 to January 2020, the ASP performed real-time PAF at the time of ordering. Appropriateness of testing was determined based on whether there was a negative result in the prior 7 days and a 3-step review of clinical factors (Fig. 1). When possible, a direct conversation took place with the ordering provider. If not possible, a general note delineating appropriate clinical criteria for testing was generated. No PAF was done outside standard hours. The ASP recommended cancelling tests deemed inappropriate. Monthly test rates during the pre- and postintervention periods were compared using the Student t test with α = .05, and test appropriateness was compared using the χ2 test. All analyses were conducted using Microsoft Excel software. Results: During the preintervention period, a total of 418 tests were ordered (104.5 per month). This number decreased to 276 (69 per month) during the intervention period. (p Conclusions: Direct PAF at the time of C. difficile PCR ordering may increase test appropriateness and is associated with a reduction in overall testing, primarily by reducing the number of tests that are considered not appropriate on clinical grounds. PAF is effective but requires significant time investment by ASP staff and may not be a sustainable intervention over time.
Funding: None
Disclosures: None

Evaluation of the genomic epidemiology and transmission of Clostridioides difficile infection across a community
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s29-s30
-
- Article
-
- You have access
- Open access
- Export citation
CLABSI
Peripheral intravascular catheter-associated bloodstream infection in the medical–surgical ICU
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s30
-
- Article
-
- You have access
- Open access
- Export citation
Blood-culture ordering practices in patients with a central line at an academic medical center–Iowa, 2020
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s30
-
- Article
-
- You have access
- Open access
- Export citation
The evaluation of central-line–associated bloodstream infection (CLABSI) preventability at an academic institution
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s30-s31
-
- Article
-
- You have access
- Open access
- Export citation
The effectiveness of a dedicated central venous access care team to prevent catheter-related bloodstream infections
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s31
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Catheter-related bloodstream infection (CRBSI) rates remain high despite the use of an insertion bundle. We hypothesized that line care and maintenance by a dedicated team would help decrease CRBSI rates. This study was conducted in The Medical City (TMC), is a 526-bed, private, tertiary-care center in Pasig City, Philippines. Methods: All adult hospitalized patients from October 1, 2020, to October 31, 2021, with a newly inserted temporary central venous catheter (CVC) were eligible for inclusion. CRBSI rates before the intervention (October 2019 to March 2020) and after the intervention (April to October 2021) were compared. The intervention arm consisted of a dedicated central venous access team (CVAT) who provided education and performed daily line care and dressing changes per protocol. A series of χ2 and Wilcoxon rank-sum tests were performed to compare characteristics between exposure groups. Incidence rates of CRBSI before and after the intervention were compared using an incidence rate ratio approach. Results: In total, 209 CVCs were enrolled in the study, with 103 CVCs (49.28%) in the preintervention arm and 106 CVCs (50.72%) in the postintervention arm. Baseline patient characteristics were similar. CRBSIs were more frequent in the preintervention arm than the postintervention arm (39 of 103 vs 28 of 106; P = .08). The CRBSI incidence density rate was higher in the preintervention arm than the postintervention arm, but the difference was not statistically significant (37.46 per 1,000 patient days vs 25.97 per 1,000 patient days; P = .14). Median time to CRBSI was similar in both groups (9 vs 8 days). Conclusions: Baseline CRBSI rates were high and risk of infection increased by day 8 after line insertion. We detected a decreasing trend in rates of CRBSI with a dedicated CVAT, but multiple interventions are likely needed to influence overall rates.
Funding: None
Disclosures: None


Hospital-acquired bloodstream infections in patients with and without hepatic failure
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s31-s32
-
- Article
-
- You have access
- Open access
- Export citation
-
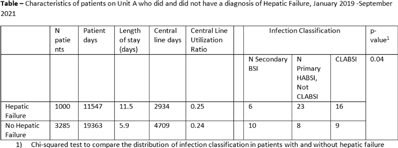
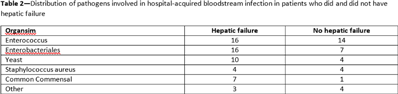
Background: The NHSN parameter estimate for predicted number of central-line–associated bloodstream infection (CLABSI) is the same for gastroenterology wards as other specialty wards, such as behavioral health and gerontology. We conducted this study to contribute to the body of knowledge surrounding the risk for hospital-acquired bloodstream infection (HABSI) in patients with and without hepatic failure. The Cleveland Clinic is a 1,200-bed, multispecialty hospital with a solid-organ transplant service. Patients with hepatic failure who do not require critical care are housed on 36-bed unit A. On unit A, 43% of patients are under hepatology or gastroenterology service, although 51% of patients are under general internal medicine. Overall, unit A has a high incidence of HABSI. Methods: Surveillance for HABSI and CLABSI is performed at the Cleveland Clinic per NHSN protocol. All patients with a midnight stay on unit A from January 2019 through September 2021 were dichotomized as having hepatic failure (yes or no) if they ever received the International Classification of Diseases Tenth Revision code for “hepatic failure, not elsewhere classified.” We joined the diagnostic code to patient days and central-line-days databases and summarized the data using Microsoft Excel software. We stratified the number of patients, patient days, device days, infection classification, and hospital length of stay by whether the patient had hepatic failure, and we compared the incidence of HABSI and CLABSI between the 2 groups using OpenEpi version 3.01 software. Results: We identified 72 HABSIs among 4,285 patients who stayed on unit A for 30,910 patient days during the study period. The incidences of HABSI in patients with and without hepatic failure were 39.0 and 13.9 per 10,000 patient days, respectively (P < .001). The incidence of CLABSI was 5.4 and 1.9 per 1,000 line days, respectively (P = .01). Patients with hepatic failure stayed longer (11.5 vs 5.9 days), yet the central-line utilization ratios were not substantially different (0.25 vs 0.24). Enterococcus was the most common pathogen involved in CLABSI in both groups (Table 2). Conclusions: Patients with hepatic failure experienced CLABSI more frequently than patients without hepatic failure, stayed longer in the hospital, and were less likely have HABSI attributed to another primary focus of infection according to NHSN definitions. Although hepatic failure may be among the most severe conditions among patients in a gastroenterology ward, we have demonstrated that these units house a population uniquely susceptible to HABSI and CLABSI.
Funding: None
Disclosures: None