Contents
Poster Presentation - Poster Presentation
Respiratory Viruses Other than SARS-CoV-2
Relevance of RSV in hospitalized adults and the need for continued testing
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s62
-
- Article
-
- You have access
- Open access
- Export citation
-
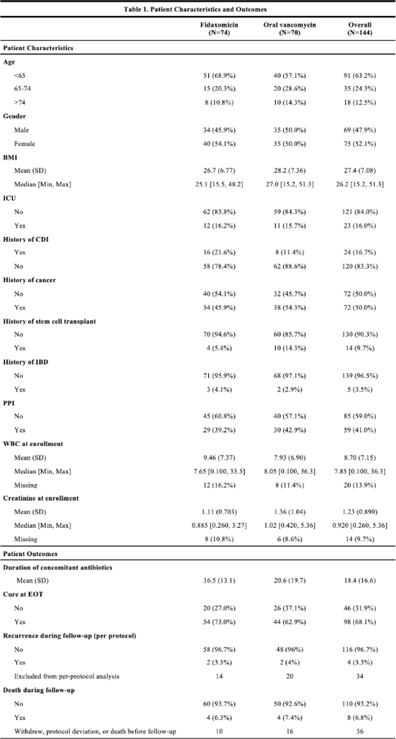
Background: RSV is underrecognized in hospitalized adults. A better understanding of RSV in this population could help prioritize targeted viral-testing resources. Hospitalization and in-hospital outcomes are widely accepted as markers of clinical severity with respect to acute respiratory illness (ARI). We compared characteristics and clinical outcomes between adults hospitalized with ARI from October 2016 through May 2019. Methods: All hospitalized adults (≥ 18 years) who met a standardized case definition of ARI were prospectively enrolled across 3 respiratory seasons from 9 hospitals participating in the US Hospitalized Adult Influenza Vaccine Effectiveness Network (HAIVEN). Demographic data were collected during enrollment interviews, and electronic medical records (EMRs) were reviewed to extract comorbidity data. Throat and nasal swabs collected at enrollment were tested for ARI pathogens using real-time PCR assays at respective HAIVEN research laboratory sites. Characteristics and clinical outcomes of participants were compared using χ2 or nonparametric tests where appropriate. Multivariable logistic regression models were used to test associations between infection status, characteristics, and clinical outcomes, adjusting for age, sex, race, Charlson comorbidity index (CCI), body mass index (BMI), site, season, and days to admission. Results: In total, 10,311 adults were included, 22.3% (n = 2,300) were aged 18–49 years, 33.2% (n = 3,423) were aged 50–64 years, and 44.5% (n = 4,588) were aged ≥65 years. Moreover, 6% of adults tested positive for RSV (n = 622), 18.8% positive for influenza (n = 1,940), and 75.1% negative for both (n = 7,749). Obesity and age ≥65 years were significantly associated with RSV detection when compared with participants negative for both RSV and influenza. Patients aged 18–49 years and ≥65 years with RSV had significantly higher median CCI scores compared to patients with influenza (Fig. 1.). The proportion of adults with CHF or COPD was significantly (p-value Conclusions: Severe RSV illness may differ from severe influenza illness, and those infected with RSV may have different characteristics than those infected with influenza. Hospitalized adults with RSV infection were more likely to have underlying cardiopulmonary comorbidities and higher CCI scores as well as experience an extended length of hospital stay and need for mechanical ventilation. These data highlight the importance of retaining testing for RSV in older adults hospitalized with ARI.
Funding: None
Disclosures: None

SSI
Feasibility and acceptability of intranasal povidone iodine decolonization among orthopedic trauma surgery patients
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s62-s63
-
- Article
-
- You have access
- Open access
- Export citation
-
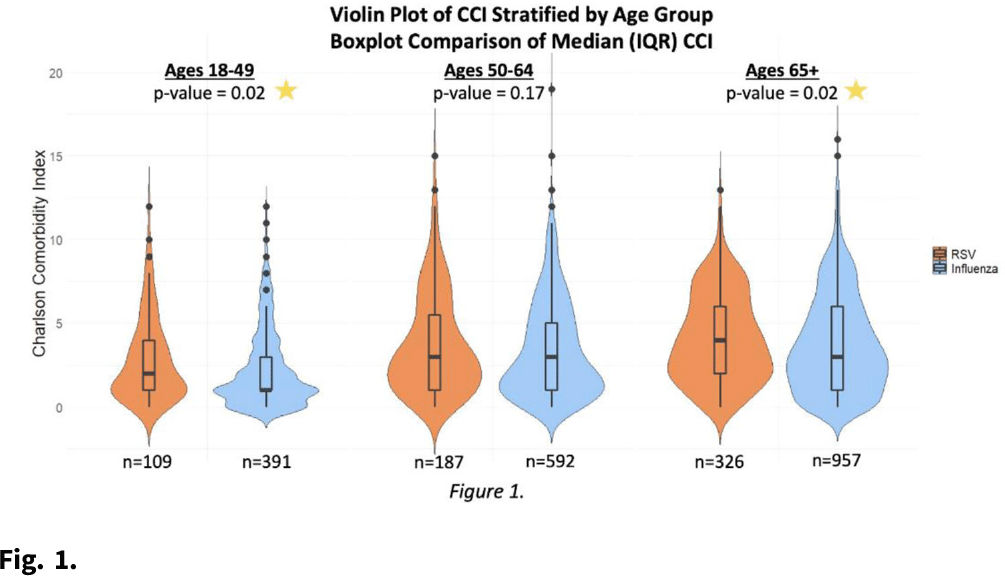
Background: Nasal decolonization significantly decreases the incidence of Staphylococcus aureus surgical-site infections (SSIs). Patient adherence with self-administration of a decolonization ointment (ie, mupirocin) is low, especially among patients having urgent surgery. Povidone-iodine decolonization may overcome patient adherence challenges because povidone-iodine needs to be applied only on the day of surgery. We assessed the effectiveness and acceptability of povidone-iodine decolonization given on the day of surgery among patients having orthopedic trauma surgery. Methods: Adult patients who underwent operative fixation of traumatic lower extremity fractures were consented to receive 10% intranasal povidone-iodine solution. Povidone-iodine was applied ~1 hour before surgical incision and was reapplied the evening after surgery. Patients were tested for S. aureus nasal colonization before surgery, the evening after surgery (before povidone-iodine reapplication), and the day after surgery. Swabs were inoculated into Dey-Engley neutralizer and processed in a vortexer. A series of dilutions were performed and plated on mannitol salt agar plates. S. aureus cultures were quantitatively assessed to determine the reduction in S. aureus after povidone-iodine use. Reductions in S. aureus nasal growth were evaluated using the Skillings-Mack test. SSIs manifesting within 30 and 90 days of surgery were identified using NHSN definitions. A survey was administered the morning after surgery to determine the acceptability of intranasal povidone-iodine. Results: In total, 51 patients participated in this pilot study between February 2020 and June 2021. Nasal samples from 12 participants (23.5%) grew S. aureus. The S. aureus concentration decreased significantly across the time points (P = .03) (Fig. 1). No SSIs were identified within 30 days of surgery. One SSI occurred within 90 days of surgery; this patient did not carry S. aureus, and cultures from the infected site were negative. Also, 31% of patients reported at least 1 mild side effect while using povidone-iodine: dripping (n = 7), itching (n = 6), dryness (n = 4), stinging (n = 4), staining (n = 3), unpleasant taste (n = 3), runny nose (n = 2), burning (n = 1), sneezing (n = 1), sore throat (n = 1), tickling (n = 1), and/or cough (n = 1). Also, 86% of patients stated that povidone-iodine felt neutral, pleasant, or very pleasant, and only 14% stated that it felt unpleasant or very unpleasant. Discussion: In this pilot study, 2 applications of nasal povidone-iodine on the day of surgery were acceptable for patients, and this protocol significantly reduced S. aureus concentration in nares of patients. Future large clinical trials should evaluate whether this 2-application regimen of povidone-iodine significantly decreases rates of SSI among orthopedic trauma surgery patients.
Funding: PDI Healthcare
Disclosures: None

Implementation of surgical site infection surveillance in 16 health facilities in Sierra Leone
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s63
-
- Article
-
- You have access
- Open access
- Export citation
Surveillance/Public Health
Increases in methicillin-sensitive Staphylococcus aureus bloodstream infection incidence, 2016–2019
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s63-s64
-
- Article
-
- You have access
- Open access
- Export citation
-
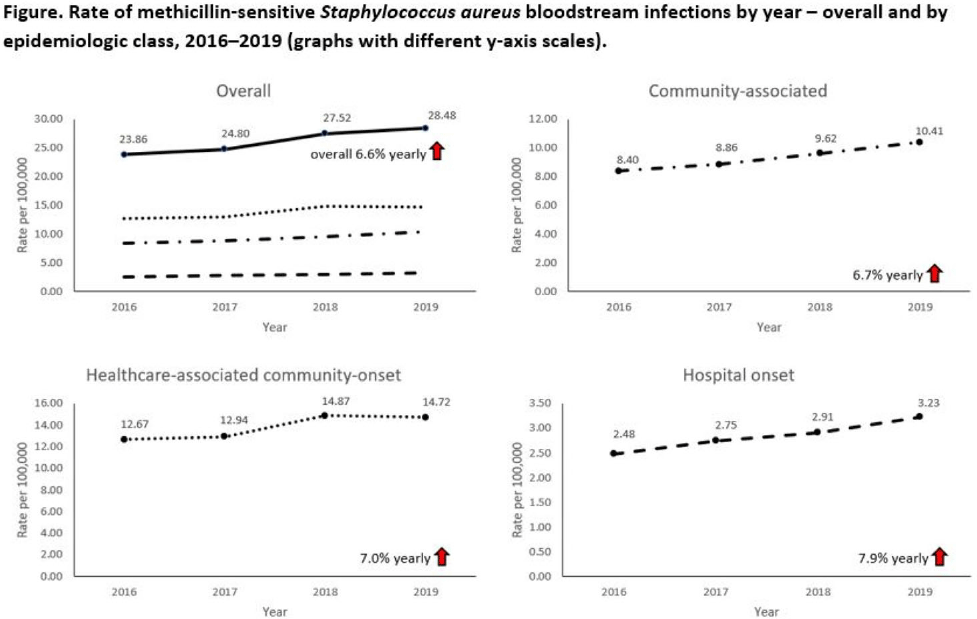
Background: Incidence of methicillin-sensitive Staphylococcus aureus (MSSA) bloodstream infections (BSIs) in the United States during 2012–2017 has been reported to have been stable for hospital-onset BSIs and to have increased 3.9% per year for community-onset BSIs. We sought to determine whether these trends continued in more recent years and whether there were further differences within subgroups of community-onset BSIs. Methods: We analyzed CDC Emerging Infections Program active, population- and laboratory-based surveillance data during 2016–2019 for MSSA BSIs from 8 counties in 5 states. BSI cases were defined as isolation of MSSA from blood in a surveillance area resident. Cases were considered hospital onset (HO) if culture was obtained >3 days after hospital admission and healthcare-associated community-onset (HACO) if culture was obtained on or after day 3 of hospitalization and was associated with dialysis, hospitalization, surgery, or long-term care facility residence within 1 year prior or if a central venous catheter was present ≤2 days prior. Cases were otherwise considered community-associated (CA). Annual rates per 100,000 census population were calculated for each epidemiologic classification; rates of HACO cases among chronic dialysis patients per 100,000 dialysis patients were calculated using US Renal Data System data. Annual increases were modeled using negative binomial or Poisson regression and accounting for changes in the overall population age group, and sex. Descriptive analyses were performed. Results: Overall, 8,344 MSSA BSI cases were reported. From 2016–2019 total MSSA BSI rates increased from 23.9 per 100,000 to 28.5 per 100,000 (6.6% per year; P < .01). MSSA BSI rates also increased significantly among all epidemiologic classes. HO cases increased from 2.5 per 100,000 to 3.2 per 100,000 (7.9% per year; P = .01). HACO cases increased from 12.7 per 100,000 to 14.7 per 100,000 (7.0% per year; P = .01). CA cases increased from 8.4 per 100,000 to 10.4 per 100,000 (6.7% per year; P < .01) (Fig. 1). Significant increases in MSSA BSI rates were also observed for nondialysis HACO cases (9.3 per 100,000 to 11.1 per 100,000; 7.8% per year; P < .01) but not dialysis HACO cases (1,823.2 per 100,000 to 1,857.4 per 100,000; 1.4% per year; P = .59). Healthcare risk factors for HACO cases were hospitalization in the previous year (82%), surgery (31%), dialysis (27%), and long-term care facility residence (19%). Conclusions: MSSA BSI rates increased from 2016–2019 overall, among all epidemiologic classes, and among nondialysis HACO cases. Efforts to prevent MSSA BSIs among individuals with healthcare risk factors, particularly those related to hospitalization, might have an impact on MSSA BSI rates.
Funding: None
Disclosures: None

Reduction in outpatient antibiotic utilization: An unintended benefit of the COVID-19 pandemic?
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s64
-
- Article
-
- You have access
- Open access
- Export citation
-
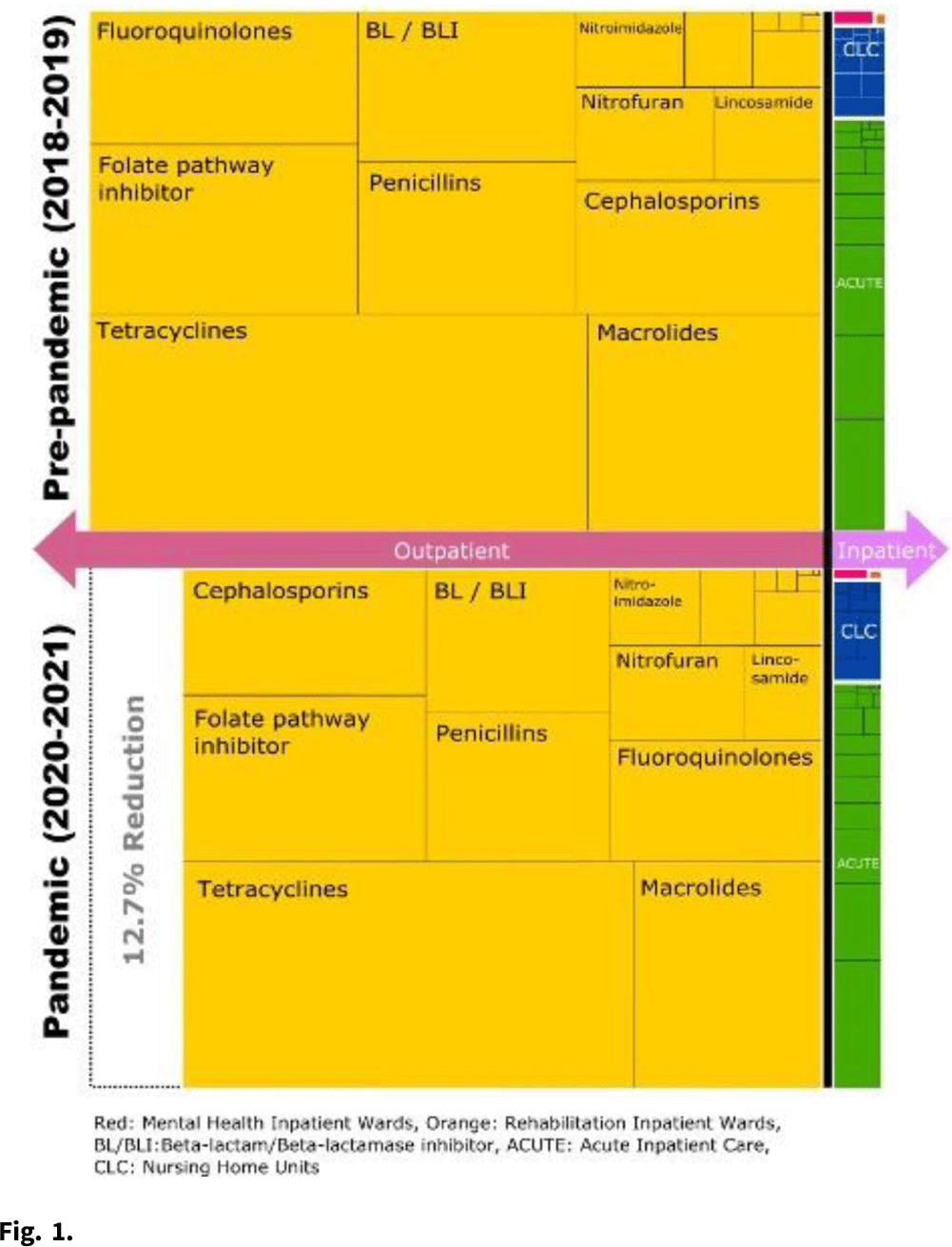
Background: The COVID-19 pandemic heavily affected healthcare delivery systems in the United States. However, little is known about its impact on overall antimicrobial consumption, especially in outpatient settings. We assessed the impact of the COVID-19 pandemic on antimicrobial consumption in both outpatient and inpatient (acute-care, long-term care, and mental health) settings in the Veterans’ Health Administration (VHA) during the 2 years before and after the start of the pandemic. Methods: We conducted a retrospective study for all patients who received care within the VHA from January 2018 to December 2021. We used antibiotic days as the primary outcome measure (days of therapy for inpatient settings and dispensed days supply for outpatient settings), and we obtained data for antimicrobial consumption from the VHA Corporate Data Warehouse. Antibiotics were categorized into classes by the NHSN protocol and included only systemic agents (oral and parenteral). We defined 2018–2019 as the prepandemic period and 2020–2021 as the pandemic period. We compared the relative and absolute difference in antibiotic consumption between the 2 periods. Results: Across all periods, 8.3 million patients received care in the VHA, and an average of 28,709,680 antibiotic days were prescribed per year. Overall, 92.9% of all antibiotic days were outpatient and 7.1% were inpatient. Total antibiotic days during the pandemic period decreased by 12.4% compared to the prepandemic period (pandemic period: 53,613,840 and prepandemic period: 61,224,878). This reduction was primarily driven by reductions in outpatient settings (relative reduction: 12.7% and absolute reduction: 7,254,880 antibiotic days over 2 years), but antibiotic days in inpatient settings decreased more modestly (relative reduction: 8.4% and absolute reduction: 356,158 antibiotic days over 2 years) (Fig. 1). When frequently prescribed antimicrobials were categorized by classes, fluoroquinolones and lincosamides showed the largest decreases (fluoroquinolones: 29.2% reduction and lincosamides: 27.2% reduction). Tetracyclines and sulfamethoxazole–trimethoprim had the smallest reductions (5.2% and 11.2%, respectively). Conclusions: Compared to the prepandemic period, the pandemic was associated with a substantial reduction in overall antibiotic consumption, especially in outpatient settings, which accounted for 95% of the overall reduction despite being outside the domain of most traditional antibiotic stewardship programs. The impact of the pandemic was most modest in the use of tetracyclines and trimethoprim–sulfamethoxazole and was most prominent in the use of fluoroquinolones and lincosamides. Further studies are required to improve the causal inference between the COVID-19 pandemic and this reduction in antibiotic consumption, as well as its impact on patient outcomes.
Funding: None
Disclosures: None

Mortality rates among non-Hispanic Black and White persons in carbapenemase-producing Enterobacterales, Tennessee, 2015–2019
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s64-s65
-
- Article
-
- You have access
- Open access
- Export citation
Developing national benchmarks for antimicrobial resistance–NHSN, 2019
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s65
-
- Article
-
- You have access
- Open access
- Export citation
-
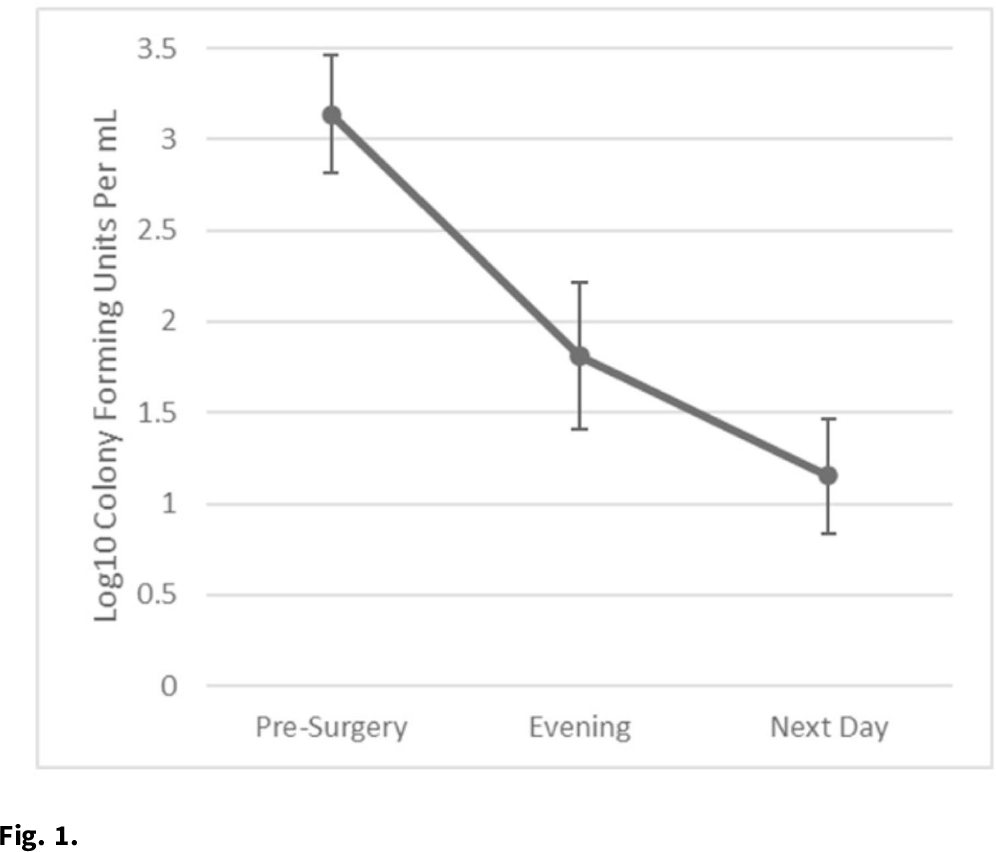
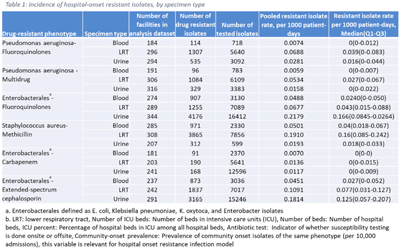
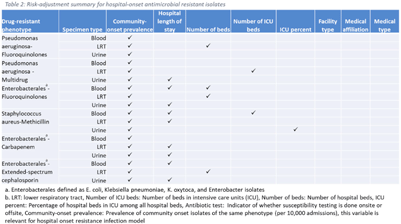
Background: The emergence and spread of drug-resistant pathogens continues to significantly impact patient safety and healthcare systems. Although antimicrobial susceptibility test (AST) results of clinical specimens are used by individual facilities for antimicrobial resistance surveillance, accurate tracking and benchmark comparison of a facility’s antimicrobial resistance using national data requires risk-adjusted methods to be more meaningful. The CDC NHSN Antimicrobial Resistance (AR) Option collects patient-level, deduplicated, isolate information, including AST results, for >20 organisms from cerebrospinal fluid, lower respiratory tract (LRT), blood, and urinary specimens. To provide risk-adjusted national benchmarks, we developed prediction models for incidence of hospital-onset isolates with antimicrobial resistance. Methods: We analyzed AST results of isolates reported through the NHSN AR Option for January through December 2019. Isolates from facilities that had >10% missing AST results for the organism-drug combinations or from hospitals that used outdated breakpoints were excluded. We assessed associations between facility-level factors and incidence rates of hospital-onset (specimen collected 3 days or more after hospital admission) isolates of specific drug-resistant phenotypes from blood, LRT, and urinary specimens. Factors included number of beds, length of stay, and prevalence of community onset isolates of the same phenotype. Drug-resistant phenotypes assessed included methicillin-resistant Staphylococcus aureus (MRSA), multidrug-resistant (MDR) Pseudomonas aeruginosa, carbapenem-resistant Enterobacterales (CRE), fluoroquinolone-resistant Pseudomonas aeruginosa, fluoroquinolone-resistant Enterobacterales, and extended-spectrum cephalosporin-resistant Enterobacterales. Isolates of different phenotypes and from different specimen sources were modeled separately. Negative binomial regression was used to evaluate the factors associated with antimicrobial resistance incidence. Variable entry into the models is based on significance level P Among the models, 1 for each drug-resistant phenotype-specimen type combination, the number of isolates with AST results ranged from 718 (Pseudomonas aeruginosa–fluoroquinolones, blood) to 16,412 (Enterobacterales–fluoroquinolones, urine). The pooled incidence rate was highest for fluoroquinolone-resistant Enterobacterales in urinary specimens (0.2179 isolates per 1,000 patient days) among all phenotype-specimen combinations evaluated (Table 1). The incidence of drug-resistant isolates was consistently associated with community-onset prevalence across models evaluated. Other associated factors varied across phenotype-specimen combinations (Table 2). Conclusions: We developed statistical models to predict facility-level incidence rates of hospital-onset antimicrobial resistant isolates based on community-onset drug-resistant prevalence and facility characteristics. These models will enable facilities to compare antimicrobial resistance rates to the national benchmarks and therefore to inform their antimicrobial stewardship and infection prevention efforts.
Funding: None
Disclosures: None


Findings from healthcare-associated infections data validation attestation in California general acute-care hospitals
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s65-s66
-
- Article
-
- You have access
- Open access
- Export citation
Lessons learned: Characteristics of first-year COVID-19 hospital outbreaks
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s66
-
- Article
-
- You have access
- Open access
- Export citation
Poster Presentation - Oral Presentation
Antibiotic Stewardship
Susceptibility results discrepancy analysis between NHSN Antibiotic Resistance (AR) Option and laboratory instrument data
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s66
-
- Article
-
- You have access
- Open access
- Export citation
Factors associated with antimicrobial drug prescription among inpatient dogs and cats at an academic veterinary hospital
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s67
-
- Article
-
- You have access
- Open access
- Export citation
Prior cultures predict subsequent susceptibility in patients with recurrent urinary tract infections
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s67
-
- Article
-
- You have access
- Open access
- Export citation
-
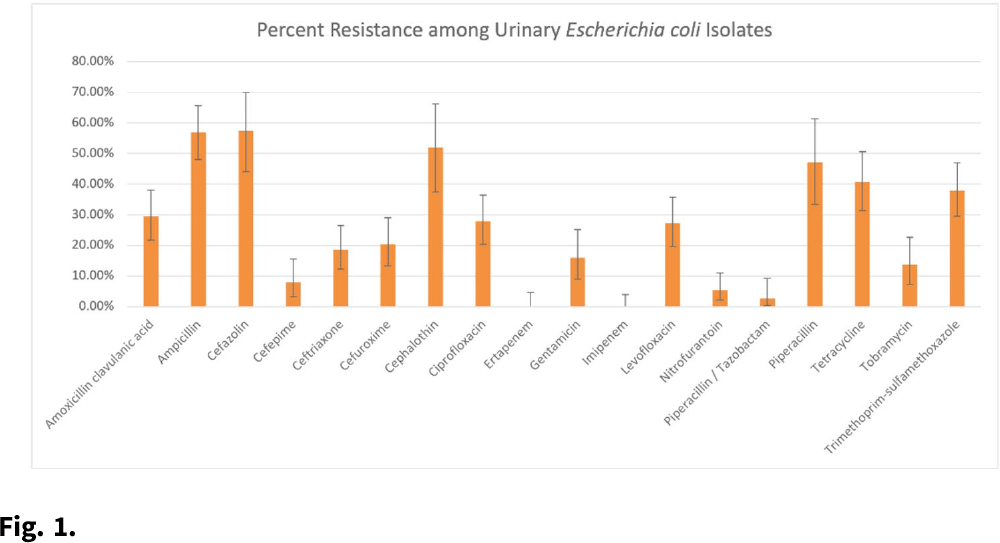
Background: Patients with recurrent urinary tract infections (rUTI) experience frequent exposure to antimicrobial regimens, leaving them at higher risk for developing antibiotic resistance. Little information on the prevalence of antibiotic resistance among patients with rUTI has been published. Although the IDSA recommends using a prior culture to guide empiric treatment, studies have not examined the predictive ability of a prior culture among patients meeting rUTI criteria. We constructed an antibiogram and evaluated test metrics, including sensitivity, specificity, and positive predictive value (PPV) and negative predictive values (NPV) of a prior culture (any organism), on predicting resistance (PPV) or susceptibility (NPV) of a future culture among patients with uncomplicated rUTI in an outpatient setting. Methods: We retrospectively extracted electronic health record data from outpatients aged ≥18 years who had an ICD-10 code for cystitis listed twice in 6 months or thrice in 12 months between November 1, 2016, and December 31, 2018. Patients sought care at either urology or primary care practices within an academic medical center in Houston, Texas. Patients with functional or structural abnormalities of the genitourinary tract, signs or symptoms of pyelonephritis, or pregnancy were excluded. Antibiogram data were reported for uropathogens with ≥30 isolates, and intermediate results were considered resistant. Test metrics and Bayes’ PPV and NPV were calculated using standard formulas. Results: We included 597 visits from 232 unique patients. Most were White (63%) and female (92%), and the cohort had a median age of 58 (IQR, 41–68). Among 310 rUTI episodes with a urine culture, 189 (61%) had at least 1 uropathogen isolated, and Escherichia coli (n = 130, 66%) was most common among all 196 uropathogens. E. coli isolates had >20% resistance to 10 of 18 antibiotics (Fig. 1). E. coli resistance to ciprofloxacin was 27.9%, resistance to nitrofurantoin was 5.5%, and resistance to trimethoprim-sulfamethoxazole was 38.0%. The PPVs for predicting resistance were highest for ceftriaxone (0.86; 95% CI, 0.60–0.96), ciprofloxacin (0.84; 95% CI, 0.63–0.94), and levofloxacin (0.84; 95% CI, 0.63–0.94). NPVs of resistance were highest for gentamicin (0.97; 95% CI, 0.83–1.00), ceftriaxone (0.94; 95% CI, 0.86–0.98), and cefepime (0.94; 95% CI, 0.84–0.98), whereas NPVs for cefuroxime, ciprofloxacin, levofloxacin, and nitrofurantoin were all >0.83. Conclusions: We detected considerable antibiotic resistance among patients with rUTI to commonly prescribed antibiotics. Prior urine culture susceptibility demonstrated moderate-to-high PPVs for predicting future resistance to ceftriaxone and fluoroquinolones as well as high NPVs for several cephalosporins and fluoroquinolones, which could inform empiric prescribing choices.
Funding: This investigator-initiated research study was funded by Rebiotix, a Ferring Company.
Disclosures: None

The effect of gender bias on acceptance of antibiotic stewardship recommendations by clinical pharmacists
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s67-s68
-
- Article
-
- You have access
- Open access
- Export citation
-
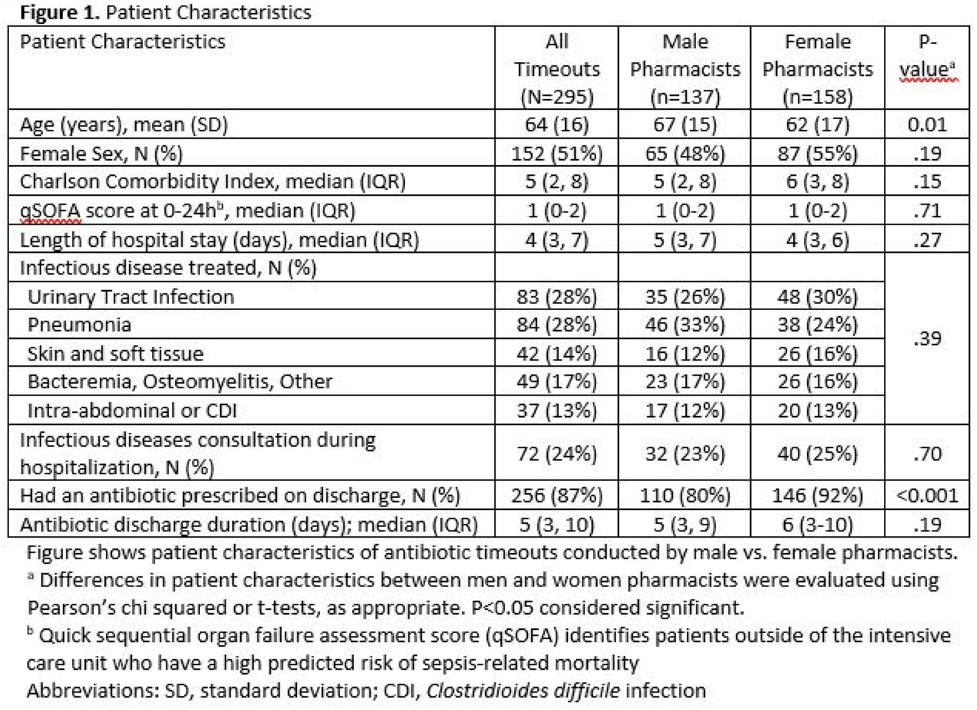
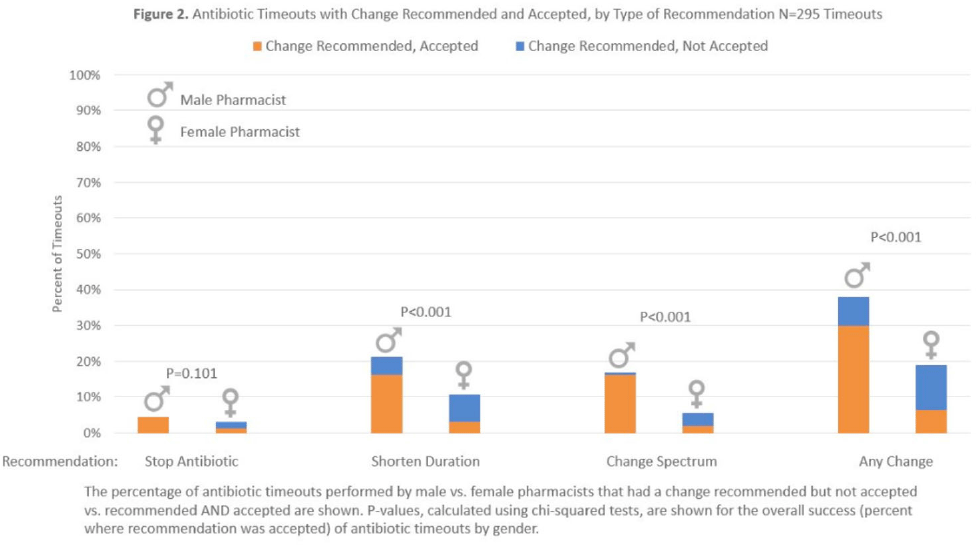
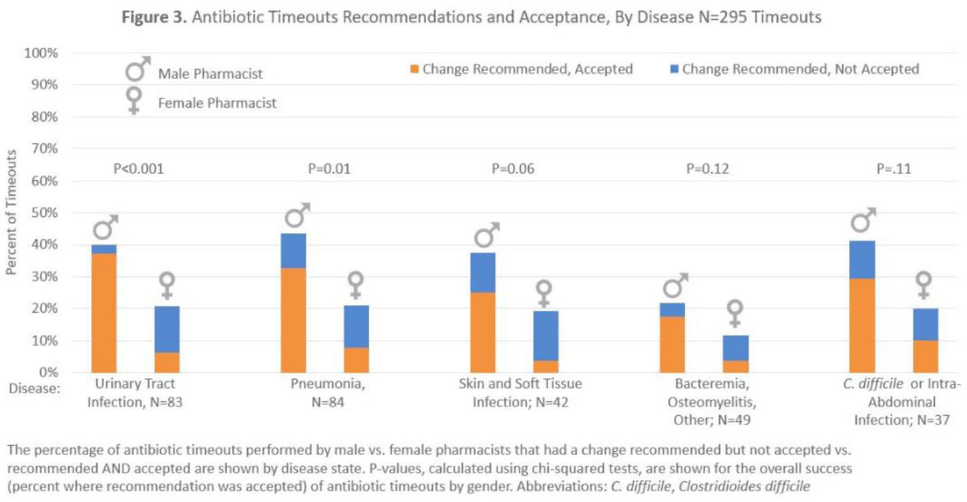
Background: Clinical pharmacists are a critical part of antibiotic stewardship. Stewardship often relies on relationships and persuasion, which may be affected by gender bias. Thus, we aimed to assess the association of sex with the acceptance of antibiotic stewardship recommendations. Methods: Between May and October 2019, medicine pharmacists at single hospital reviewed patients on antibiotics and–when a discharge was anticipated–led an antibiotic discussion (or “timeout”) prior to discharge. To explore differences in antibiotic timeout effectiveness by gender, we assessed the association of pharmacist sex with suggestion and acceptance of antibiotic changes using logistic regression controlling for patient characteristics. We also assessed whether hospitalist sex was associated with or moderated the effect of pharmacist sex on acceptance of timeout recommendations. Results: Between May 1, 2019, and October 31, 2019, pharmacists conducted 295 timeouts (patient characteristics in Fig. 1). Overall, 54% of timeouts were conducted by 12 female pharmacists and the remaining 46% were conducted by 8 male pharmacists. Overall, 82 (29%) of 295 timeouts resulted in a pharmacist recommending an antibiotic change, and male pharmacists were more likely to recommend a change: 52 (38%) of 137 versus 30 (19%) 158 (P Conclusions: In this discharge antibiotic intervention, timeouts conducted by women were less likely to result in an antibiotic change than those conducted by men. The difference in effectiveness resulted both from female pharmacists being less likely to recommend a change and from hospitalists being less likely to accept recommendations from a female pharmacist. These findings suggest that gender bias may play a role acceptance of antibiotic stewardship recommendations, which could affect antibiotic use, pharmacist job satisfaction, and patient outcomes.
Funding: None
Disclosures: None



Identifying symptoms/illnesses and situations that predispose outpatients to use antibiotics in two healthcare systems
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s68-s69
-
- Article
-
- You have access
- Open access
- Export citation
-
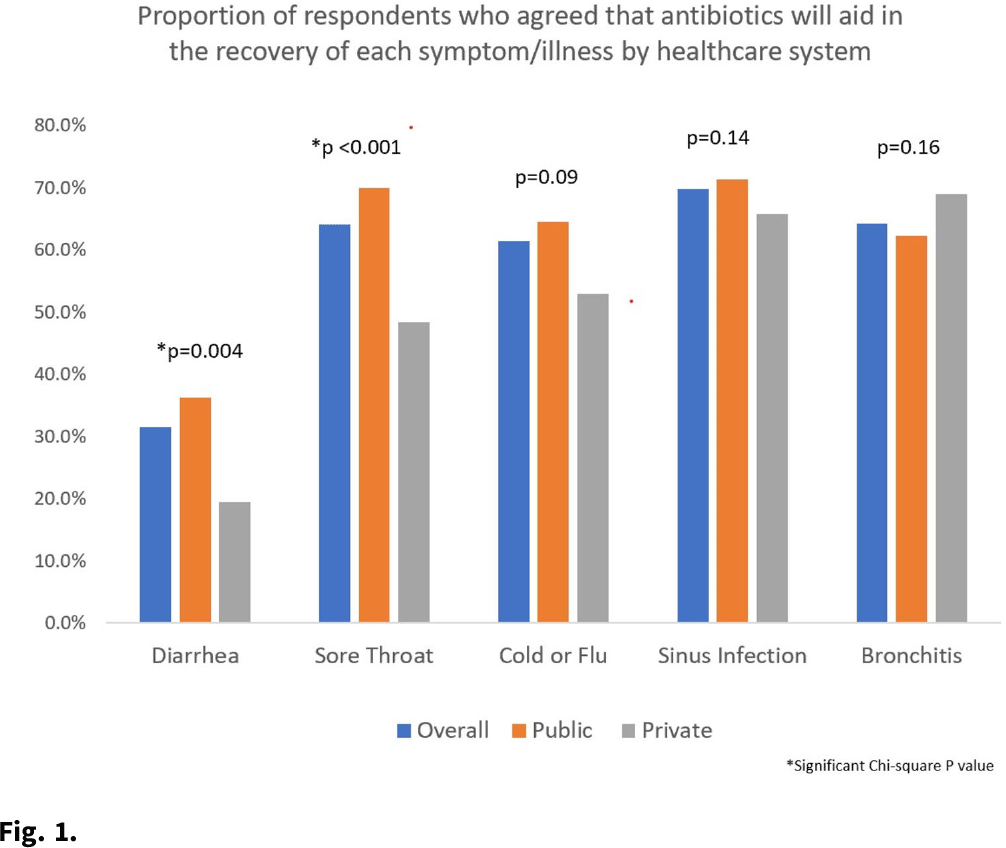
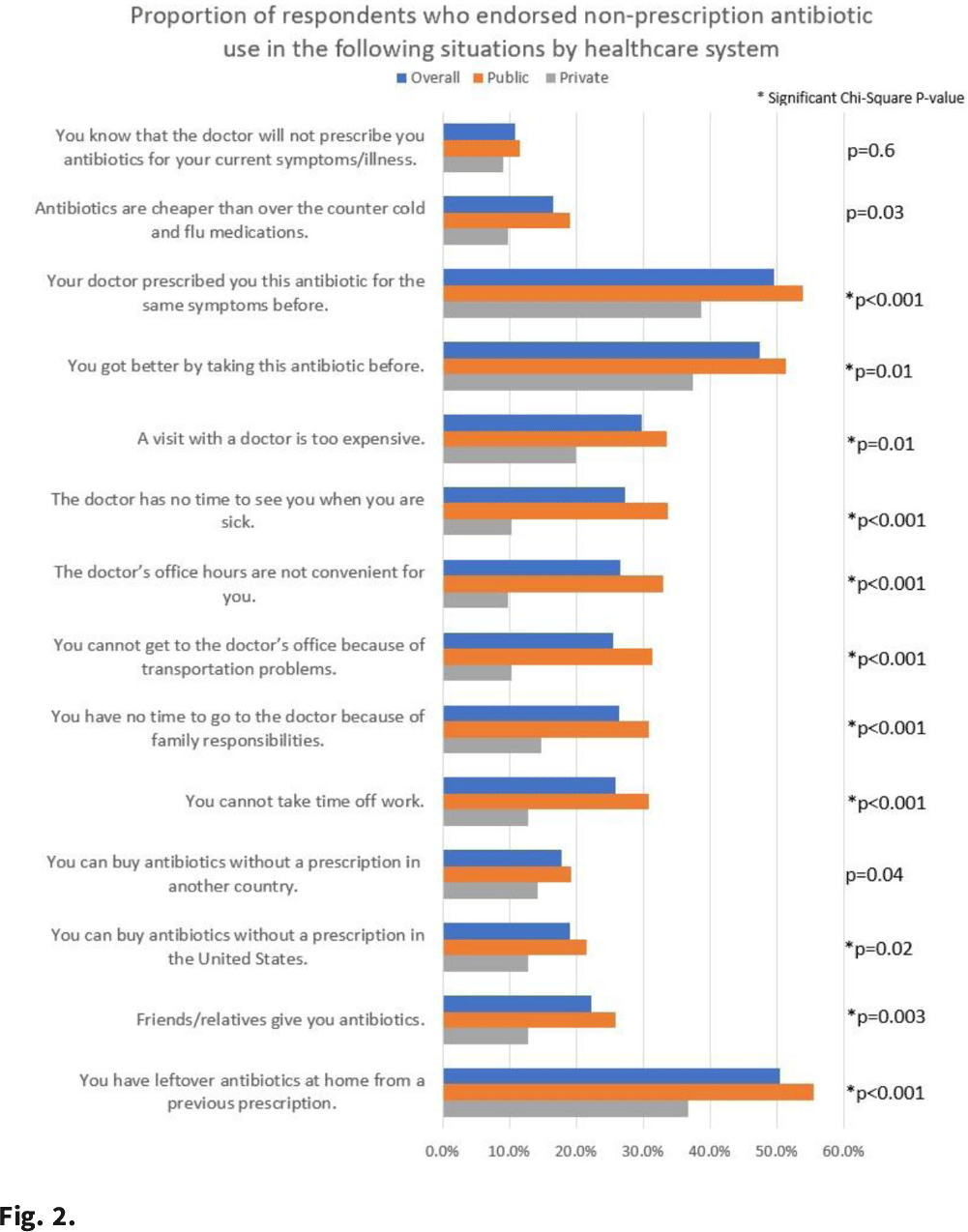
Background: Taking antibiotics outside the guidance of a clinician (nonprescription use) is a potential safety issue and runs counter to antibiotic stewardship efforts. We identified the symptoms and illnesses and situations that may predispose patients to take antibiotics, and we compared these findings between patients attending public primary care clinics and private emergency departments. Methods: A cross-sectional survey was conducted between January 2020 and March 2021 in 6 primary care clinics and 2 emergency departments in the United States. We queried patients about 5 symptoms and illnesses (Fig. 1) and 14 situations (Fig. 2) to investigate whether these would lead the patients to take antibiotics without a prescription. We used the χ2 test to compare the symptoms and illnesses and situations between the respondents from public and private healthcare systems. We set the P value for significance at <.025. Results: In total, the survey had 564 respondents (median age, 49.7 years; range, 19–92), and 72% were female. Most respondents identified as either Hispanic or Latina/Latino (46.6%) or African American or Black (33%), followed by White (15.8%), and other (4.6%). Most respondents had visited public clinics (72%). The most common insurance status for our respondents included Medicaid or county financial assistance program (56.6%), followed by private insurance or Medicare (36.7%) and self-pay (6.7%). In public primary care clinics, only 23% had private insurance or Medicare compared to 72.9% in private emergency departments. Of those surveyed, 69% agreed that antibiotics would improve the recovery from sinus infections, followed by bronchitis (64%), sore throat (64%), cold/flu (61.4%), and diarrhea (31.5%). The proportions of respondents who believed that antibiotics would improve the recovery from diarrhea (36.2% vs 19.4%; P = .004) and sore throat (59.9% vs 48.4%; P < .001) were significantly higher among public versus private outpatient respondents. We did not find significant differences for cold/flu, sinus infection, or bronchitis between these 2 healthcare systems (Fig. 1). In 11 of the 14 situations, patients in public clinics were more likely to report a likelihood of using nonprescription antibiotics than the patients visiting the private emergency rooms (Fig. 2). Conclusions: Future stewardship interventions should be aware of the symptoms and illnesses and situations that may influence outpatients to take nonprescription antibiotics. Addressing modifiable factors (eg, leftover antibiotics, antibiotics given by friends or family, and antibiotics available without a prescription in stores or markets) may also curtail these unsafe practices and reduce antibiotic resistance.
Funding: None
Disclosures: None


Using machine learning to predict antibiotic resistance to support optimal empiric treatment of urinary tract infections
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s69
-
- Article
-
- You have access
- Open access
- Export citation
-
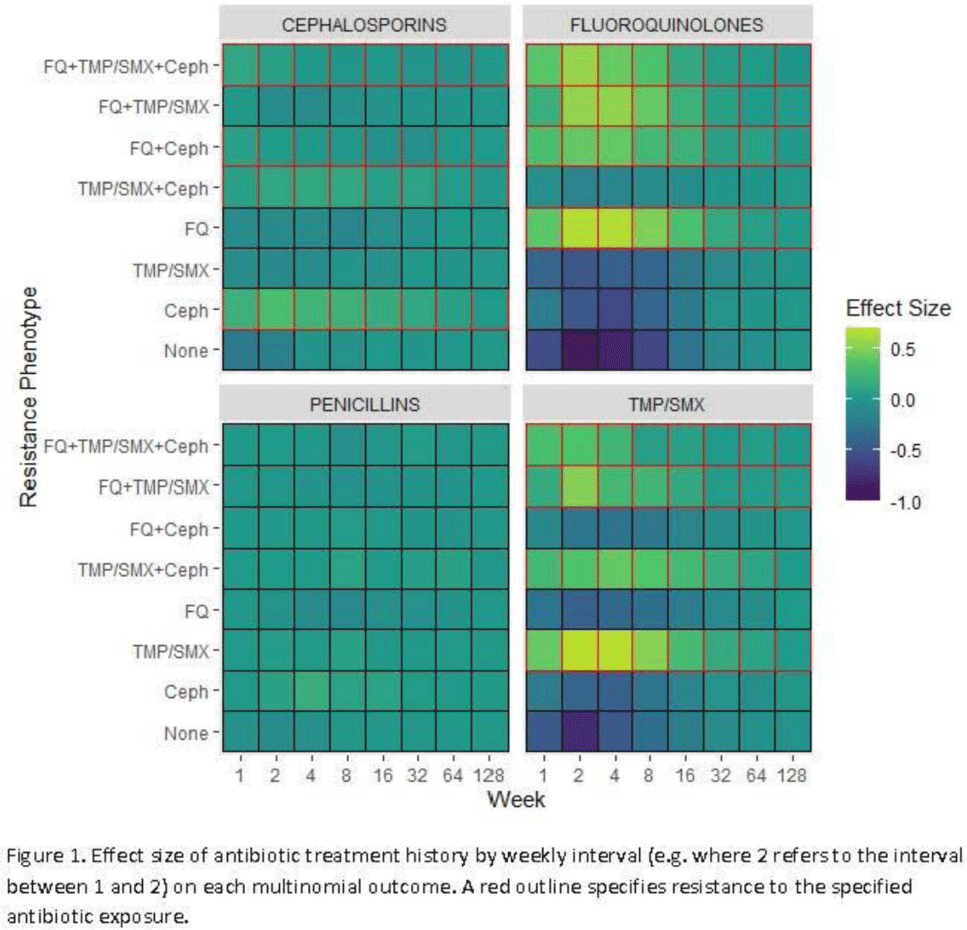
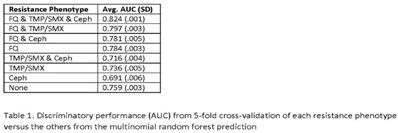
Background: Antibiotic resistance is pervasive in the Veterans’ Affairs (VA) healthcare system, with rates of fluoroquinolone and trimethoprim–sulfamethoxazole (TMP/SMX) resistance approaching 30% in E. coli urinary isolates. The efficacy of antimicrobial treatment is critically dependent on the susceptibility of the infecting pathogen; however, prescription decisions are often made empirically in practice. We analyzed susceptibility profiles of enteric gram-negative rods (Enterobacterales) from clinical urine cultures collected from ambulatory patients receiving care in VA clinics and emergency departments. Our goals were (1) to develop a predictive model to support choice of empiric antibiotics pending results of susceptibility testing and (2) to examine the relationship between past antibiotic exposures and susceptibility profiles to enhance understanding of antibiotic selective pressure. Methods: We obtained 265,076 positive cultures from 157,422 unique patients from 2015 to 2020. We trained random forest multinomial classifiers to estimate the risk of a positive urine culture isolate being resistant to the multinomial outcome: fluoroquinolone, TMP–SMX, cephalosporin, or any combination of these 3 agents. Data sources evaluated for model generation included demographics, comorbidities, trend and seasonal terms, treatment history for multiple antimicrobial treatments summarized using number of prescriptions in weekly intervals, and sample history summarized by number of resistant and susceptible cultures in weekly intervals. Using 5-fold cross validation, we assess the performance of the clinical prediction using the area under the receiver operating characteristic curve (AUC) for each multinomial outcome. In addition to prediction, we modeled the direct effect of treatment on resistance using multinomial group lasso (MGL). This method allows variable selection in variable groupings, such as all variables related to the fluoroquinolone treatment history, which allowed us to assess the effect of a patient’s complete course of treatment on resistance. Results: In cross-validation analysis, our random forest model was best at predicting outcomes with fluoroquinolone resistant phenotypes compared to non–fluoroquinolone-resistant phenotypes (Table 1). From MGL, we found that having a prescription for fluoroquinolone treatment 4–8 weeks prior to a urinalysis was positively associated with fluoroquinolone resistance and negatively associated with fluoroquinolone susceptible phenotypes (Fig. 1). Conclusions: Our results show that a patient’s sample and treatment history are highly predictive of a future resistance. Fluoroquinolone treatment is especially associated with increased risk of fluoroquinolone single- and multidrug resistances. A history of either fluoroquinolone or trimethoprim-sulfamethoxazole (TMP-SMX) treatment is a stronger indicator of a future resistant phenotype than cephalosporin or penicillin.
Funding: None
Disclosures: None


Private practice dentists improve antibiotic use after dental antibiotic stewardship from infectious diseases experts
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s70
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Dentists prescribe ~25.7 million antibiotic prescriptions annually. Private practice dentists (PPDs) represent 80% of US dentists who need to implement dental antimicrobial stewardship. We conducted a prospective cohort study of PPDs comparing appropriateness of antibiotic use before and after dental AS education. Methods: PPDs were invited to participate in this study. In phase 1 (pre-education), we collected 3 months (June–August 2019) of retrospective antibiotic use data (indication, dose, duration, penicillin allergy history) and number of dental procedures. We also conducted a preliminary survey to assess baseline antimicrobial stewardship knowledge. In phase 2 (education), PPDs attended 4 televideo education sessions (March–May 2021) taught by an infectious disease– antimicrobial stewardship (ID-AS) pharmacist and physician. In phase 3 (posteducation), we prospectively collected 3 months (June–August 2021) of antibiotic use data (as in phase 1), using an online database with ongoing feedback. In phase 4, we conducted antibiotic use audit and feedback to PPDs after the survey, and we solicited recommendations to reach more PPDs. The Student t test was used for statistical analyses. Results: Study participants comprised 15 PPDs: 2 oral maxillofacial surgeons, 6 periodontists, 4 endodontists, and 3 general dentists. Among them, 10 had been in practice >20 years. The presurvey revealed that 14 were unfamiliar with dental antimicrobial stewardship. All prescribed clindamycin (25% for nonpenicillin allergy), and standard antibiotic duration ranged from 5 to 14 days based on dental school training. In phase 3, despite more procedures, overall antibiotic use and duration decreased, and the use of clindamycin, quinolones, and prophylaxis for joint implant patients, also decreased. Appropriate use improved from 22% to 95%. Postsurvey responses on perceived value of antimicrobial stewardship education were 100% positive, with recommendations to make antimicrobial stewardship a required annual continuing education, similar to opioid continuing education. Study participants invited the ID-AS experts to teach an additional 150 PPDs to date via established PPD study clubs to expand dental antimicrobial stewardship across the United States. Conclusions: After learning dental antimicrobial stewardship guidance from ID-AS experts, PPDs rapidly optimized antibiotic prescribing behavior. PPDs identified their established study clubs as a forum to quickly expand dental antimicrobial stewardship training by ID-AS experts throughout the United States.
Funding: MERCK
Disclosures: None


Metrics in outpatient stewardship: Is more always better?
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s70-s71
-
- Article
-
- You have access
- Open access
- Export citation
-
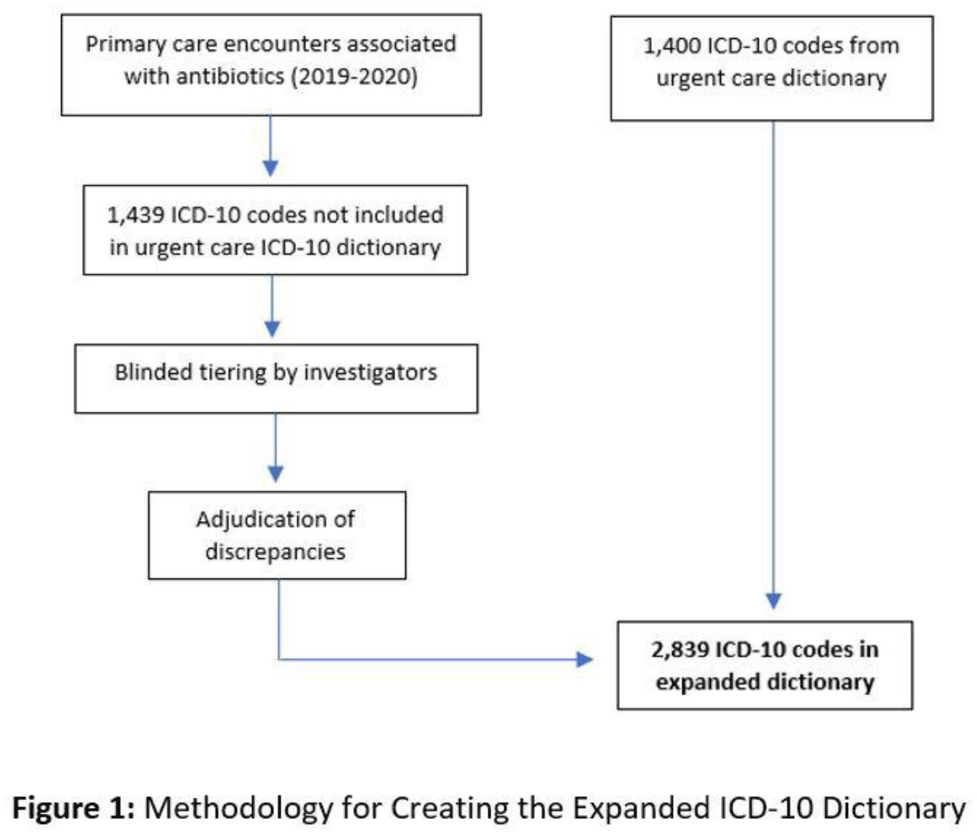
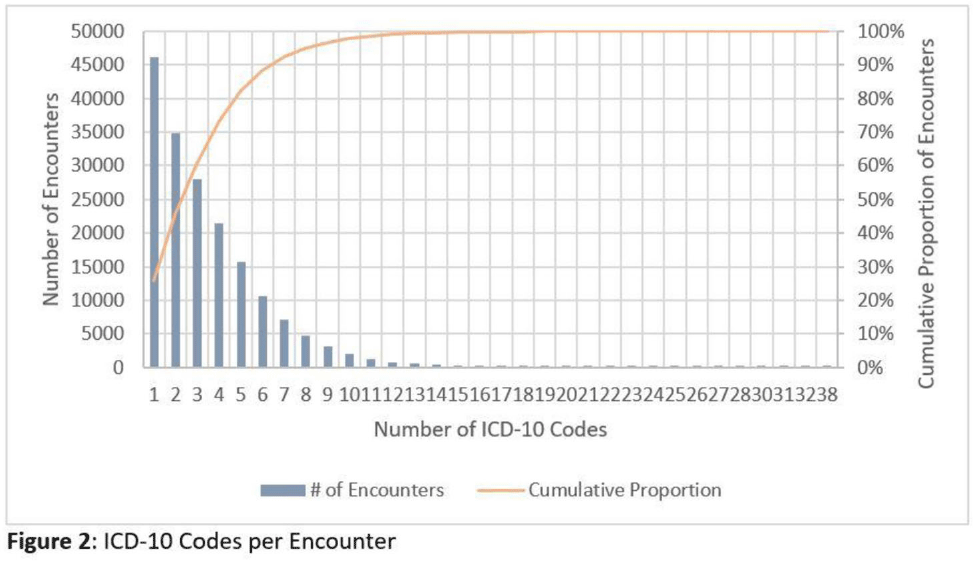
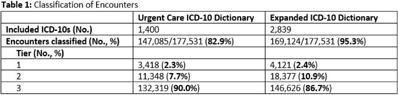
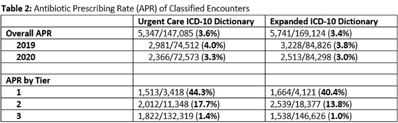
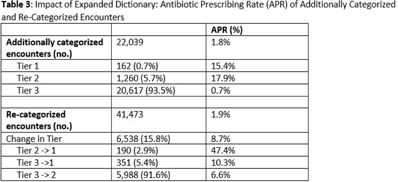
Background: Emerging evidence supports the use of billing data to identify stewardship targets in primary care. Standardizing an approach to antibiotic prescribing rate (APR) calculations could facilitate external benchmarking. Methods: Using methodology and an ICD-10 dictionary validated in urgent care clinics,1 we created an expanded ICD-10 dictionary to incorporate additional ICD-10 codes from primary care associated with antibiotic prescriptions (Fig. 1). We then compared antibiotic prescribing rates using the urgent care and expanded dictionaries. We included all primary care visits from 2019 to 2020 and extracted ICD-10 codes and antibiotic order data. Using the urgent care and expanded ICD-10 dictionary, we classified each encounter by prescribing tier based on whether antibiotics are almost always (tier 1), sometimes (tier 2), or almost never (tier 3) indicated. For encounters with ICD-10s in multiple tiers, we chose the lowest tier. For multiple ICD-10 codes within the same tier, we chose the first extracted ICD-10 code. We calculated antibiotic prescribing rates as the proportion of encounters associated with ≥ 1 antibacterial prescription. This quality improvement project was deemed non–human subjects research by the Stanford Panel on Human Subjects in Medical Research. Results: The urgent care dictionary has 1,400 ICD-10 codes. We added 1,439 ICD-10 codes derived from primary care encounters to create the expanded ICD-10 dictionary (8.5% tier 1, 9.1% tier 2, and 82.4% tier 3) (Fig. 1). We identified 177,531 encounters; 74% had ≥ 2 associated ICD-10 codes (Fig. 2). In total, 147,085 encounters (82.9%) were classified into a tier using the urgent care dictionary. An additional 22,039 encounters were classified with the expanded dictionary (Table 1). Most added encounters were tier 3 with low 0.7% APR (Tables 1 and 3). In total, 41,473 (28.2%) encounters were classified differently depending on the ICD-10 dictionary used, most commonly changing from tier 3 to tier 2 without an increase in overall tier 2 antibiotic prescribing rate (Tables 2 and 3). Overall antibiotic prescribing rates were similar when using either the urgent care or expanded ICD-10 dictionary (Table 2). Conclusions: The expanded ICD-10 dictionary allowed for classification of more encounters in primary care; however, it did not meaningfully change antibiotic prescribing rates. Antibiotic prescribing rates were likely diluted by classifying more encounters without identifying an associated increase in antibiotic prescribing. A more sophisticated classification system may help to accommodate the diversity and volume of ICD-10 codes used in primary care.
1. Stenehjem E, et al. Clin Infect Dis 2020;70:1781–1787.
Funding: None
Disclosures: None





Evaluation of periprocedure antibiotics and infection-related hospitalizations after transrectal prostate biopsies
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s71
-
- Article
-
- You have access
- Open access
- Export citation
Rates of intravenous antibiotic starts among outpatient hemodialysis patients using NHSN dialysis event reporting, 2016–2020
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s71-s72
-
- Article
-
- You have access
- Open access
- Export citation
-
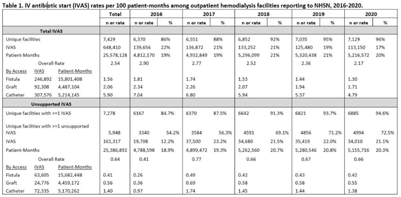
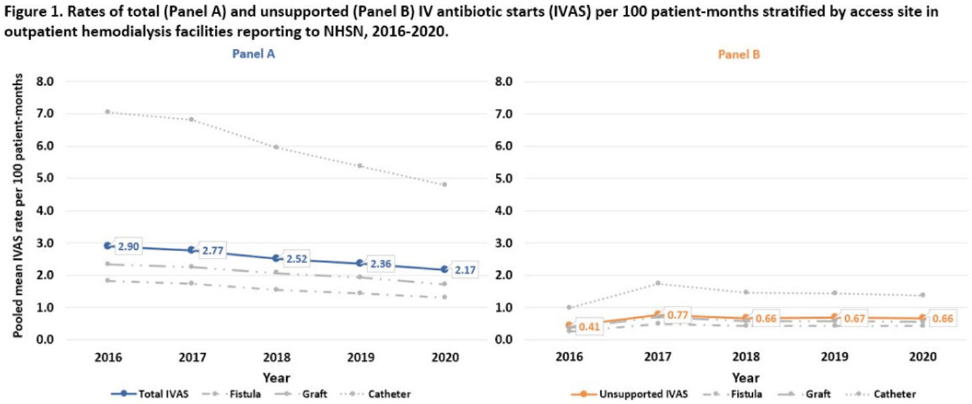
Background: Nearly one-third of patients on hemodialysis receive intravenous (IV) antibiotics annually, but national data characterizing antibiotic use in this population are limited. Using NHSN surveillance data for outpatient dialysis facilities, we estimated temporal changes in the rate of IV antibiotic starts (IVAS) among hemodialysis patients as well as the proportion of IVAS that were not supported by a reported clinical indication. Methods: IVAS events were obtained from the NHSN Dialysis Event module between 2016 and 2020, excluding patients who were out of network, receiving peritoneal or home dialysis, or with unspecified vascular access. IVAS unsupported by documentation were defined as new IVAS without a collected or positive blood culture, pus, redness or swelling event, or an associated clinical symptom. Pooled mean rates of total and unsupported IVAS were estimated per 100 patient months yearly and stratified by vascular access type. Differences in IVAS rates by year were estimated with negative binomial regression. Results: Between 2016 and 2020, 7,278 facilities reported 648,410 IVAS events; 161,317 (25%) were unsupported by documentation (Table 1). In 2016, 3,340 (54%) facilities with ≥1 IVAS event reported an IVAS unsupported by documentation, which increased to 4,994 (73%) in 2020. Total IVAS rates decreased by an average of 8.2% annually (95% CI, 7.1%–9.3%; P < .001). The average annual percentage decrease did not differ significantly by vascular access site. The total IVAS rate was lowest in 2020 (2.17 per 100 patient months; 95% CI, 2.18–2.17). IVAS rates in 2020 were greatest for patients with catheter access (4.79 per 100 patient months; 95% CI, 4.75–4.83), followed by graft (1.71 per 100 patient months; 95% CI, 1.68–1.73), and lowest for patients with fistulas (1.30 per 100 patient months; 95% CI, 1.29–1.31). The overall pooled mean rate of unsupported IVAS was 0.64 per 100 patient months (95% CI, 0.63–0.64), which did not significantly change by year (Fig. 1). Conclusions: Total IVAS rates among outpatient hemodialysis patients have decreased since 2016, and rates among catheter patients remain highest compared to patients with fistulas or grafts. However, unsupported IVAS rates did not change, and the proportion of facilities reporting an unsupported IVAS increased annually. Targeted efforts to engage facilities with unsupported IVAS may help improve accurate reporting and prescribing practices.
Funding: None
Disclosures: None


C. difficile
Comparison of fidaxomicin to oral vancomycin for the treatment of Clostridioides difficile infection in hospitalized patients
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s72-s73
-
- Article
-
- You have access
- Open access
- Export citation
-
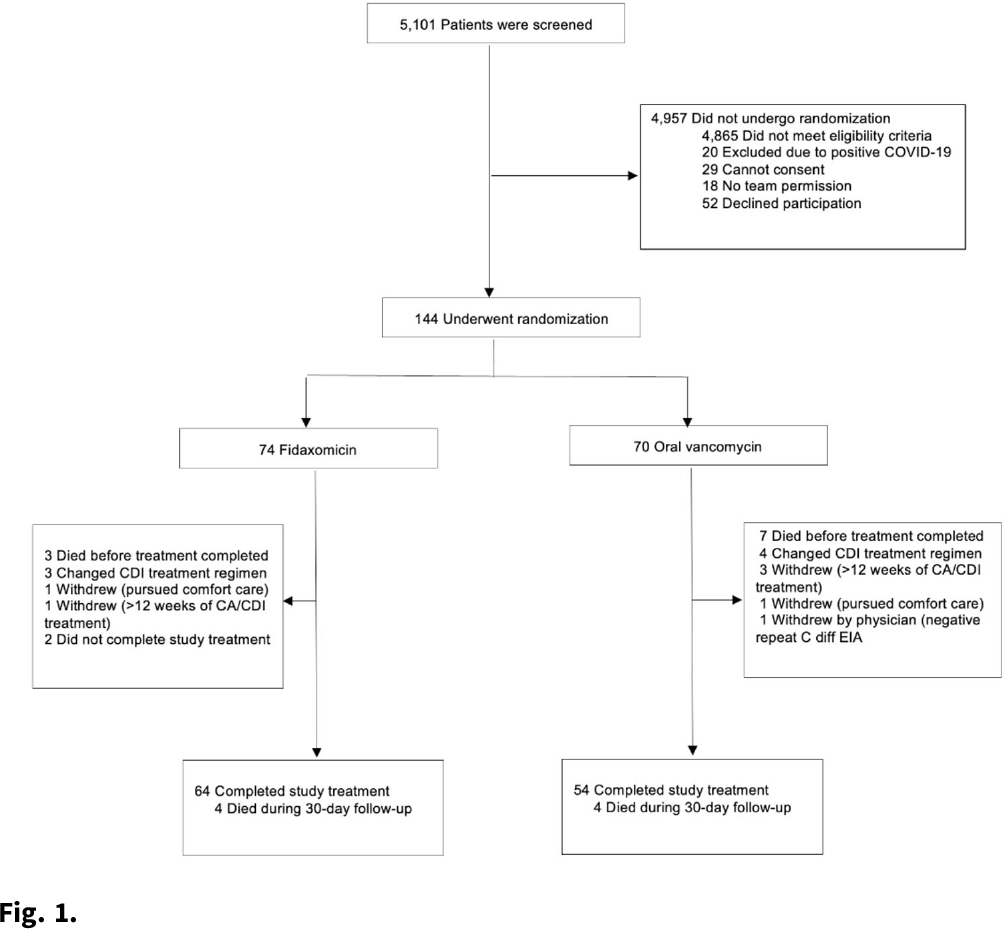
Background:Clostridioides difficile infection (CDI) is a major source of morbidity and mortality. Even after recovery, recurrent CDI (rCDI) occurs frequently, and concomitant antibiotic use for treatment of a concurrent non–C. difficile infection is a major risk factor. Treatment with fidaxomicin versus vancomycin is associated with similar rate of cure and lower recurrence risk. However, the comparative efficacy of these 2 agents remains unclear in those receiving concomitant antibiotics. Methods: We conducted a randomized, controlled, open-label trial at the University of Michigan and St. Joseph Mercy hospitals in Ann Arbor, Michigan. Patients provided written informed consent at enrollment. We included all hospitalized patients aged ≥18 years with a positive test for toxigenic C. difficile, >3 unformed stools per 24 hours, and ≥1 qualifying concomitant antibiotic with a planned treatment of an infection for ≥5 days after enrollment. We excluded patients with complicated CDI, allergy to vancomycin–fidaxomicin, planned adjunctive CDI treatments, CDI treatment for >24 hours prior to enrollment, concomitant laxative use, current or planned colostomy or ileostomy, and/or planned long-term (>12 weeks) concomitant antibiotic use. Clinical cure was defined as resolution of diarrhea for 2 consecutive days maintained until the end of therapy and for 2 days afterward. rCDI was defined as recurrent diarrhea with positive testing within 30 days of initial treatment. Patients were randomized (stratified by ICU status) to fidaxomicin 200 mg twice daily or vancomycin 125 mg orally 4 times daily for 10 days. If concomitant antibiotic treatment continued >10 days, the study drug continued until the concomitant antibiotic ended. Bivariable statistics included t tests and χ2 tests. Results: After screening 5,101 patients for eligibility (May 2017–May 2021), 144 were included and randomized (Fig. 1). Study characteristics and outcomes are noted in Table 1. Baseline characteristics were similar between groups. Most patients were aged <65 years, were on a proton-pump inhibitor (PPI), and were not in the ICU. The mean duration of concomitant antibiotic was 18.4 days. In the intention-to-treat population, clinical cure (73% vs 62.9%; P =.195), and rCDI (3.3% vs 4.0%; P >.99) were similar for fidaxomicin and vancomycin, respectively. Conclusions: In this study of patients with CDI receiving a concomitant antibiotic, a numerically higher proportion were cured with fidaxomicin versus vancomycin, but this result did not reach statistical significance. Overall recurrence was lower than anticipated in both arms compared to previous studies in which duration of CDI treatment was not extended during concomitant antibiotic treatment. Future studies are needed to ascertain whether clinical cure is higher with fidaxomicin than vancomycin during concomitant antibiotic exposure, and whether extending the duration of CDI treatment reduces recurrence.
Funding: Merck & Co.
Disclosures: None