Contents
Poster Presentation - Poster Presentation
COVID-19
assessment of Vaccine Interest in Unvaccinated COVID-19–positive inpatients
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s42
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Although vaccine hesitancy has been an issue for many years, it has become a major point of contention in the effort to mitigate the COVID-19 pandemic. In August 2021, a large academic medical facility began capturing the vaccination status of admitted COVID-19–positive patients, as well as their interest in the COVID-19 vaccine. We performed a descriptive analysis on the characteristics of unvaccinated patients who contracted COVID-19 and their interest in receiving the COVID-19 vaccine. Methods: Patient history and physical (H&P) notes and demographic data were collected using the internal data warehouse sourced from the electronic medical record for all SARS-COV-2–positive inpatient admissions to UNC Medical Center and UNC Chatham from August 1, 2021, to January 11, 2022. Manual chart reviews of progress notes were completed for patients whose history was not recorded in the initial H&P. Demographic data were summarized by vaccine status overall and by interest in COVID-19 vaccine among unvaccinated patients. We performed χ2 to determine demographic differences between the interested and uninterested unvaccinated groups. Results: In total, 536 patients were admitted with COVID-19 from August 1, 2021, to January 11, 2022. Of these, 15% were fully vaccinated (2 doses mRNA plus 1 dose J&J); 5.4% were partially vaccinated; 75.7% were unvaccinated; and 2.9% had an unknown vaccination status. Demographic characteristics are presented in Table 1. The most common demographics were consistent among the fully vaccinated and unvaccinated groups, with the exception of sex and age group (Table 1). For those whose interest data were available (n = 164), 34% were uninterested in receiving the COVID-19 vaccine. Importantly, race and age were statistically significantly different (P < .05) between the unvaccinated interested and unvaccinated uninterested groups. Conclusions: Even after experiencing COVID-19 firsthand and being hospitalized, some people who remain uninterested in receiving the COVID-19 vaccine. This population had a statistically higher proportion of white and older individuals than the unvaccinated interested group. Recommendations from healthcare providers might not be effective in persuading this population to be vaccinated. Instead, grassroots alternatives might be more successful. Additional analysis should be considered on whether patients who expressed interest in COVID-19 vaccine received immunization.
Funding: None
Disclosures: None

Stay home, save lives: Characterizing sickness presenteeism and motives among healthcare personnel in the COVID-19 pandemic
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s42
-
- Article
-
- You have access
- Open access
- Export citation
Care innovations and health disparities: An exploration of COVID-19 outcomes in inpatient and hospital-at-home care settings
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s43
-
- Article
-
- You have access
- Open access
- Export citation
-
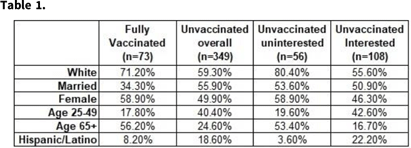
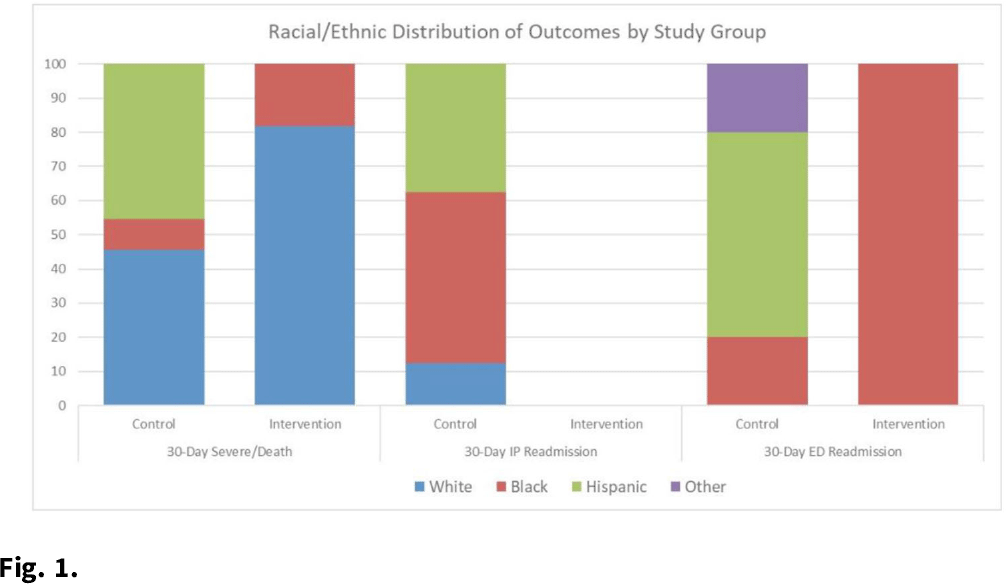
Background: Hospital at home (HaH) programs have been a critical resource for providing inpatient care to acutely ill patients throughout the COVID-19 pandemic. Given that this innovative care delivery model relies on technology and environmental concerns, questions have been raised about the effectiveness of HaH for vulnerable groups. However, evidence is extremely limited regarding equity issues in the HaH context. Thus, we explored COVID-19 outcomes within vulnerable groups. Methods: We conducted a matched, retrospective study of 116 acutely ill patients with COVID-19, aged ≥18 years, who presented to an AH emergency department (ED) and were admitted for inpatient care. Treatment patients were admitted to AH HaH between July 15 and September 31, 2020, and control patients were hospitalized between May 8 and June 25, 2020. Patients were matched based on oxygen requirement and DS CRB-65 (DEFINE) score. Race or ethnicity and area deprivation index (ADI) were chosen as predictors of health disparities. The ADI incorporates 17 indicators of poverty, educational attainment, and housing quality at the census tract level. Outcomes included 30-day (from discharge) severe illness or death composite, IP readmission, and ED visit. Results: The frequency of 30-day severe illness or death and ED visits were equivalent between the groups (n = 11; ED n = 5); the proportion of severe illness was higher for White patients in AH-HaH (n = 9 vs n = 5), and for Hispanic patients treated in the hospital (n = 5 vs n = 0; Fig. 1). There were no 30-day inpatient readmissions in the AH-HaH group, but 8 readmissions occurred with inpatients. The distribution of severe illness among the ADI quintiles varied. For traditional inpatients, disease progression was limited to ADI Q3–5 (Q3 = 3, Q4 = 6, Q5 = 2); for AH-HaH patients, disease progression was not influenced by ADI. The effect of ADI on 30-day ED readmission was nonsignificant. Conclusions: Although exploratory in nature, the results suggest that HaH may help combat sources of health disparities that have dominated the pandemic. Although inpatient care resulted in inpatient readmissions, mainly among Black and Hispanic patients, AH-HaH stays were not associated with any inpatient readmissions. The equivalent distribution among ADI quintiles of patients who became severely ill within 30 days of their AH-HaH stay suggests that HaH may be able to leverage innovation to reach vulnerable populations and reduce the impact of factors that contribute to inequity.
Funding: None
Disclosures: None

Decolonization Strategies
Indwelling medical devices and skin microorganisms on ICU patients bathed with chlorhexidine gluconate
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s43-s44
-
- Article
-
- You have access
- Open access
- Export citation
-
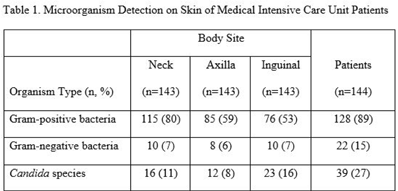
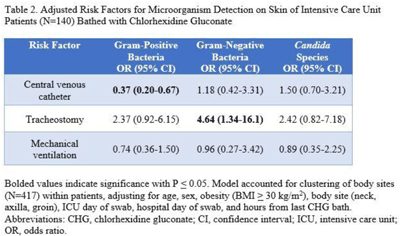
Background: Bathing ICU patients with chlorhexidine gluconate (CHG) decreases bloodstream infections and multidrug-resistant organism transmission. The efficacy of CHG bathing on skin microorganism reduction may be influenced by patient-level clinical factors. We assessed the impact of clinical factors on the recovery of microorganisms from the skin of patients admitted to an ICU who were receiving routine CHG bathing. Methods: We analyzed data obtained from 6 single-day point-prevalence surveys of adult ICU patients between January and October 2018 at 1 medical ICU, in the context of a CHG bathing quality initiative. Demographics and covariates were collected at the bedside and by chart review. Skin swabs were collected from neck, axilla, and inguinal regions and were plated to selective and nonselective media. Standard microbiologic methods were used for species identification and susceptibilities. Multivariable models included patients who received a CHG bath and accounted for clustering of body sites within patients. Results: Across all time points, 144 patients participated, yielding 429 skin swab samples. Mean age was 57 years (SD, 17); 49% were male; 44% had a central venous catheter; and 15% had a tracheostomy Also, 140 patients (97%) had >1 CHG bath prior to skin swab collection, with a median of 9 hours since their last CHG bath (IQR, 6–13 hours). Gram-positive bacteria were more commonly recovered than gram-negative or Candida spp across all skin sites (Table 1). Variation by body site was detected only for gram-positive bacteria, with recovery more common from the neck compared to axilla or groin sites. On multivariate logistic regression (Table 2), presence of central venous catheter was associated with lower odds of gram-positive bacteria recovery among those who received a CHG bath. Presence of tracheostomy was associated with a significantly higher odds of gram-negative bacteria detection on skin. No clinical factors were independently associated with recovery of Candida spp. Conclusions: Central venous catheter presence was associated with lower odds of gram-positive bacteria detection on skin, suggesting the possibility of higher quality CHG bathing among such patients. Tracheostomy presence was associated with greater odds of gram-negative bacteria detection, suggesting that it may be a potential reservoir for skin contamination or colonization. Indwelling medical devices may influence CHG bathing effectiveness in reducing microorganism burden on skin.
Funding: None
Disclosures: None


Diagnostic/Microbiology
Assessment of the effects of rapid diagnostic biofire blood culture identification panel in hospitalized patients
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s44
-
- Article
-
- You have access
- Open access
- Export citation
The impact of GenMark Dx ePlex blood-culture identification on the treatment and outcomes of gram-positive bacteremia
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s44
-
- Article
-
- You have access
- Open access
- Export citation
-
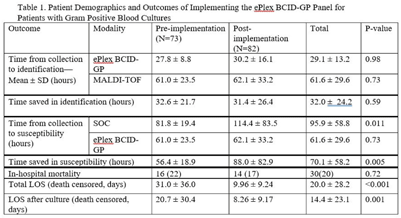
Background: In the treatment of bloodstream infections, the identification of the causal pathogen, and the evaluation of its susceptibility to antibiotics, often serve as the rate-limiting steps of the patient’s hospital stay. The GenMark Dx ePlex blood culture identification gram-positive (BCID-GP) panel aims to alleviate this bottleneck, thereby reducing the risk of severe complications and the spread of resistance, using electrowetting technology to detect the most common causes of GP bacteremia (20 targets) and 4 antimicrobial resistance (AMR) genes. We hypothesized that implementation of the ePlex BCID-GP panel would improve antimicrobial choice and de-escalation where appropriate. Methods: A mixed blinded and unblinded study was conducted to assess the effect of the BCID-GP panel on the outcomes and antibiotic stewardship of GP bacteremic patients before ePlex results were made clinically available (before implementation, N = 73) and once they accompanied the standard-of-care work-up (after implementation, N = 82). Differences in time to different benchmarks between the 2 modalities and the effect on patient outcomes were analyzed using null-hypothesis significance testing. Results: During the study, the BCID-GP panel identified 63 (42%) Staphylococcus epidermidis isolates, 31 (21%) Staphylococcus spp, 24 (16%) Staphylococcus aureus isolates, 12 (8%) Streptococcus spp, and 7 (5%) Enterococcus spp, and results were similar in the pre- and postimplementation groups (P = .13). The panel saved an average of 32.0 ± 24.2 hours in pathogen identification over standard-of-care methods, with no statistical difference made by the clinical availability of the data (Table 1). In terms of susceptibility testing, the panel saved an average of 70.1 ± 58.2 hours but with less unity between the 2 cohorts (P = .005). Of the 66 cases with follow-up, identification via ePlex indicated an escalation of therapy in 20 (30%) and a narrowing of coverage in 31 (47%). In patients identified to have Staphylococcus aureus, BCID-GP could change antimicrobial therapy in 79%; the need for escalation of antibiotics was identified in 58% of cases. In patients with Staphylococcus epidermidis bacteremia, implementation of BCID-GP panel could have resulted in de-escalation of antimicrobial therapy in 67% of patients. The implementation of the BCID-GP panel was correlated with no significant change of in-hospital mortality (P = .72) but was correlated with a significantly decreased death-censored total length of stay (LOS) (P < .001) and LOS after culture (P = .001). Conclusions: Our study has demonstrated that nonculture identification of bacteria and susceptibility can result in major improvements in antimicrobial therapy in patients, particularly those with contaminants identified.
Funding: GenMark DX
Disclosures: None

Disinfection/Sterilization
Measuring the impact of an enhanced strategy for daily disinfection in acute-care hospital rooms
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s45
-
- Article
-
- You have access
- Open access
- Export citation
-
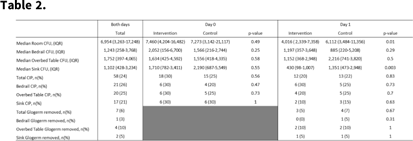
Background: Enhanced strategies for daily disinfection in acute-care hospital rooms are needed but are poorly understood. Methods: We conducted a randomized control trial pilot study in acute-care hospital rooms at Duke University Health System in Durham, North Carolina, comparing the efficacy of a novel EPA-registered quaternary ammonium disinfectant with 24-hour activity, Sani24, to routine daily disinfection. Rooms housing patients on contact precautions were enrolled. In each study room, the bedrails, overbed table, and sink were divided into 2 equal halves, or sides, labeled left and right, with sample areas of 2,000 cm2, 1,750 cm2, and 400 cm2, respectively. Each sample area side was then randomized 1:1 to intervention or control by a coin toss. Sani24 was applied to the surface of each intervention sample side and allowed to air dry. Control sides were left alone. Environmental services (EVS) staff were not involved in the study and were blinded to randomization status. Glogerm dots were applied to all 6 sample-area sides after application of the intervention to measure compliance of daily disinfection by EVS and the removal of the intervention agent. Microbiological samples were taken with sponges premoistened with neutralizing buffer from each sample area side for 6 total samples (3 intervention and 3 control) immediately before and 24 hours following application of the intervention agent. Clinically important pathogens (CIP) were defined as MRSA, VRE, and CRE. The primary outcome was room CFU on study day 1, which was compared using a Wilcoxon rank-sum test. Results: In total, 20 patient rooms were enrolled in the study, and 240 samples were obtained from 120 sites (60 intervention and 60 control) from November 2021 to January 2022. Enrolled patients were all on contact isolation and had an active infection; 15 (75%) were bedridden and 8 (40%) were female. On day 0, baseline contamination was similar between study arms: 7,460 (IQR,4,204–16,482) room CFU and 18 samples (30%) harboring CIP in the intervention arm versus 7,273 (IQR, 3,142–21,117) and 15 samples (25%) in the control arm (P = .49 and .47, respectively). On day 1, intervention areas had significantly lower CFU at 4,016 (IQR, 2,339–7,358) compared to controls at 6,112 CFU (IQR, 3,484–11,356; P = .01). No significant differences were detected between study arms regarding CIP recovery. Glogerm was minimally removed from sample areas (n = 7, 3%), and the result was similar between study arms. Conclusions: The use of the quaternary ammonium disinfectant with 24-hour activity on high-touch healthcare surfaces led to reduced contamination over a 24-hour period. Routine daily disinfection compliance by EVS was low since minimal sample areas had Glogerm removed
Funding: PDI
Disclosures: None

Assessment of cleaning stethoscopes using UV-C sanitation
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s45-s46
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: It is well established that stethoscopes harbor pathogenic bacteria species. Within hospital settings, these pathogens can be rapidly transmitted from room to room and can cause harm in vulnerable populations. The current literature demonstrates that disinfecting stethoscopes with isopropanol kills 99% of all bacteria. However, in practice this rarely occurs and disinfection is subject to user error. We assessed the efficacy of ultraviolet germicidal irradiation (UV-C) at decontaminating stethoscopes used at our rural healthcare system along with the cleaning habits of their users. Methods: Stethoscopes were randomly selected from the clinical staff of our hospital’s largest nursing unit. The stethoscopes were each swabbed for culture then exposed to UV-C for 20 seconds and sampled again. Users were asked to complete a survey during this process. Samples were then cultivated on tryptone soya broth (TSB) agar, and all growth was sent for identification via matrix-assisted laser desorption/ionization (MALDI-TOF). Later, the protocol was repeated to assess cleaning efficacy of the isopropanol wipes commonly used in our hospital. We collected pre- and postintervention samples after cleaning vigorously for 3 minutes according to the manufacturer’s guidelines. The samples were classified as follows: “cleaner” if the number of colonies decreased after sanitation, “sterilized” if the number of colonies decreased to zero, “no change” if the number of colonies stayed the same, and “no assessment” if there was no preintervention growth. Several samples “increased” in CFU count after the intervention, likely due to incomplete sampling, contamination, or incomplete penetration of UV-C. The Fisher exact test was used to analyze the effectiveness of the stethoscope sanitation techniques. Results: In total, 60 samples (33 used for analysis) were obtained from stethoscopes cleaned with UV-C (Fig. 1). Moreover, 34 samples (28 used for analysis) were obtained from stethoscopes cleaned with isopropanol (Fig. 2). Both UV-C (93.9% vs 6.1%; P < .01) and isopropanol (100% vs 0%; P < .01) resulted in a significant decrease in bacterial colonization on stethoscopes. UV-C was not more effective at sanitizing stethoscopes than isopropanol (93.9% vs 100%; P = .50). Conclusions: Both UV-C and isopropanol were effective at cleaning hospital stethoscopes. Given that UV-C is not subject to user error and that it takes less time to clean a stethoscope than isopropanol, it may be the superior option in a clinical setting.
Funding: None
Disclosures: None




Hand Hygiene
Hand hygiene adherence at entrances and exits of healthcare facilities in two rural districts of Uganda
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s46
-
- Article
-
- You have access
- Open access
- Export citation
Compliance and constraints of hand hygiene among healthcare workers in Bangladesh
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s46-s47
-
- Article
-
- You have access
- Open access
- Export citation
-
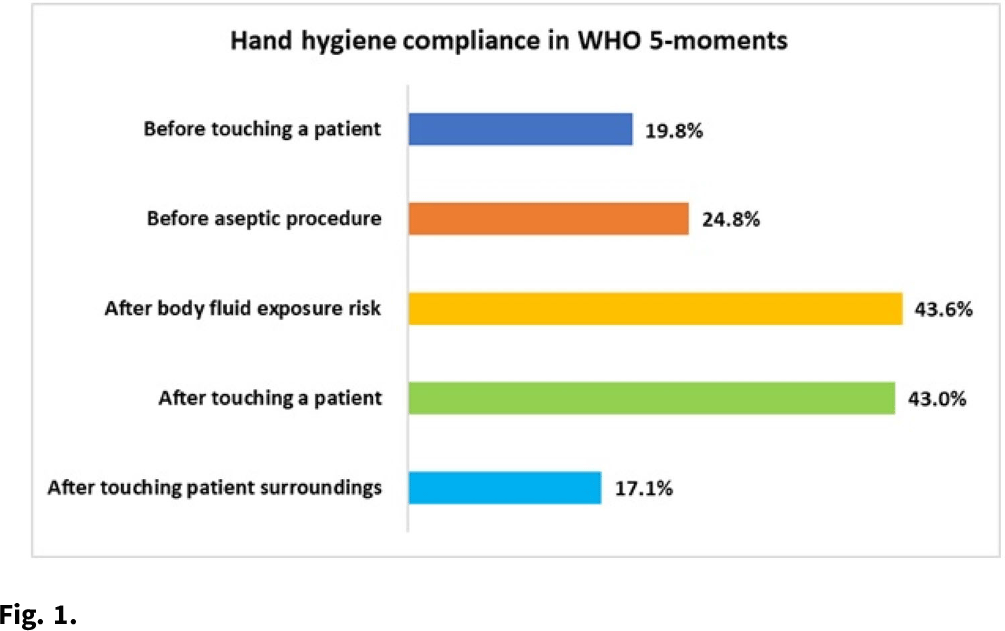
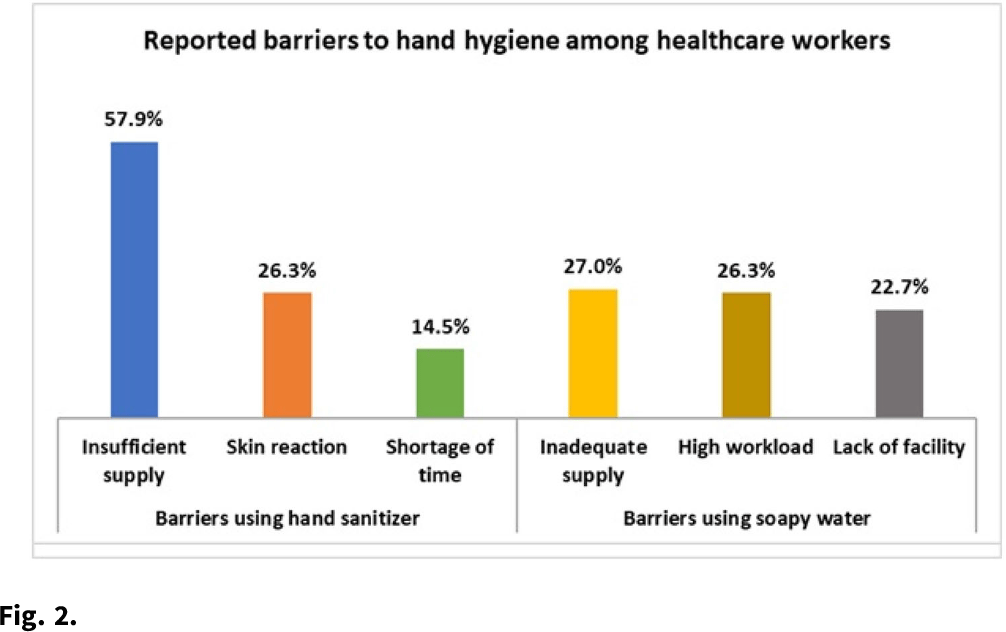
Background: Hand hygiene (HH) is a core element of patient safety and the single most essential strategy for preventing healthcare-associated infections (HAIs). Adherence to HH among healthcare workers (HCWs) varies greatly depending on a range of factors, including risk perceptions, institutional culture, auditing mechanisms, and availability of HH supplies. We observed HH compliance among HCWs to determine the factors influencing practices in tertiary healthcare facilities in Bangladesh. Methods: During September 2020–February 2021, we conducted nonparticipatory observations at 11 tertiary-care hospitals in Bangladesh using the WHO “Five Moments for Hand Hygiene” tool to record compliance among physicians, nurses, and cleaning staff. We also performed semistructured interviews to determine the key barriers to complying with hand hygiene. Furthermore, we noted the presence, location, and functionality of existing HH stations within each hospital ward. Results: We observed 14,668 HH opportunities among HCWs. The overall HH compliance was 25.3%, and compliance differed significantly by professional category (P < .001). Physicians had the highest HH compliance at 28.5% (2,264 of 7,930), followed by nurses at 25.4% (1,272 of 5,008). Cleaning staff had the lowest rates of HH at 9.9% (171 of 3,221). HCWs of public hospitals had significantly higher odds of complying with HH practices than those in private hospitals (27.4% vs 17.9%; aOR, 1.73; 95% CI, 1.55–1.93; P < .001). HH compliance also varied by WHO Five Moments indicators. HCWs were 3 times more likely to perform HH ‘after touching a patient’ than ‘before touching patient’ (aOR, 3.36; 95% CI, 2.90–3.90; P < .001). Common barriers to using hand sanitizer were insufficient supply (57.9%), skin reaction (26.3%), shortage of time (14.5%), and lack of awareness (11.9%). Regarding handwashing with soap, inadequate supplies (27.0%), high workload (26.3%), and lack of facilities (22.7%) were the key factors for low adherence. The HH infrastructure observation in 82 wards showed that running water and soap were available in 168 (86.2%) of 195 HCW-designated basins, compared to 51 (35.9%) of 142 for the patient- and attendant-assigned basins. Handwashing posters were found in only 44 (13.1%) of 337 basin surroundings, and no hand drying supplies were observed for patients or attendants. Conclusions: Hand hygiene compliance among HCWs fall significantly short of the standard for safe patient care. Inadequate HH supplies in a resource-constrained setting like Bangladesh demonstrates a lack of leadership in prioritizing, promoting, and investing in infection prevention and control. The findings of this study might help to motivate and design interventions for HH compliance, which will help reduce HAIs in the hospital setting.
Funding: None
Disclosures: None


Electronic hand hygiene monitoring systems: Perceptions and behaviors
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s47
-
- Article
-
- You have access
- Open access
- Export citation
Local production of alcohol-based hand rub to optimize hand hygiene facility in healthcare settings during COVID-19
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s47-s48
-
- Article
-
- You have access
- Open access
- Export citation
-
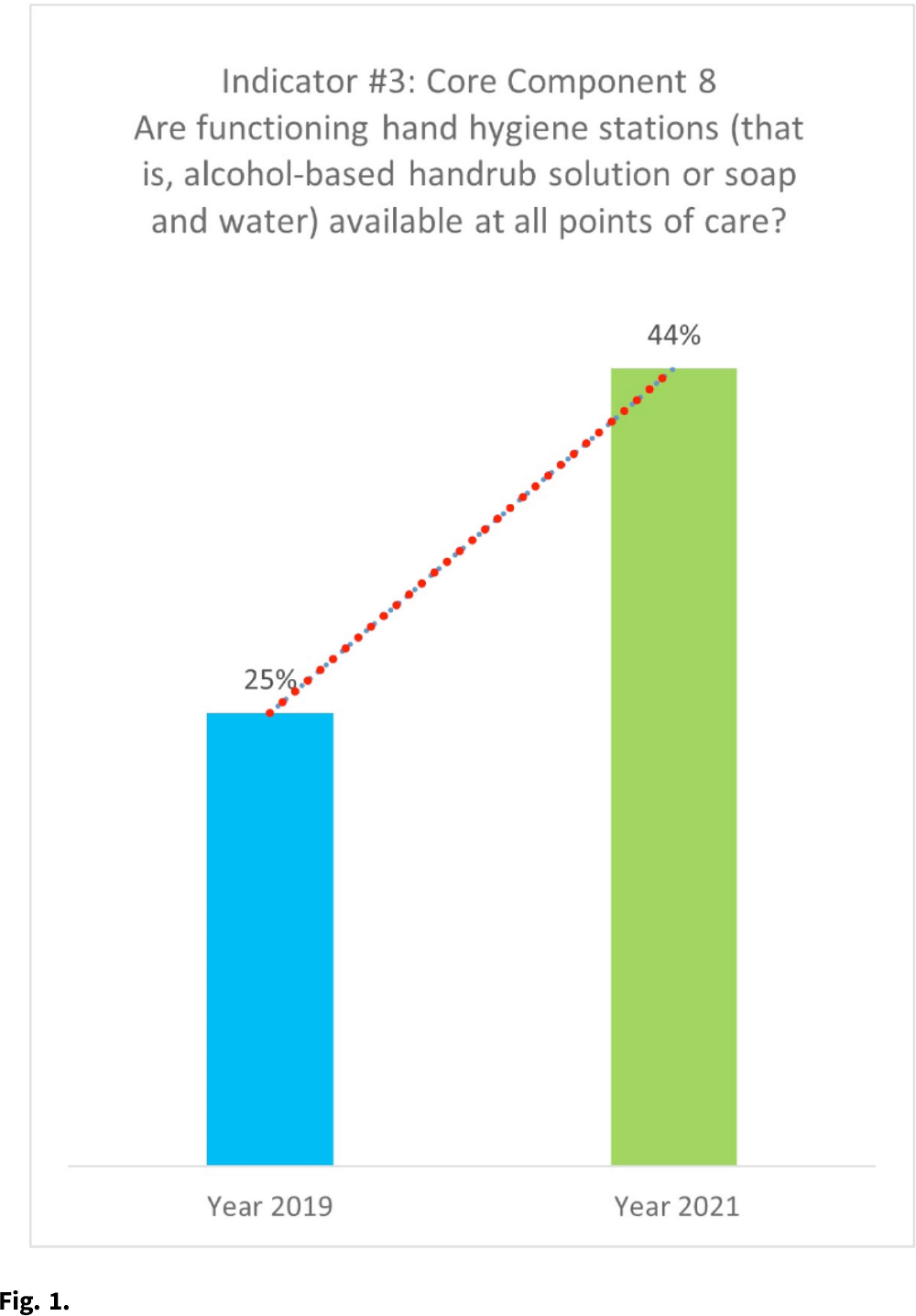
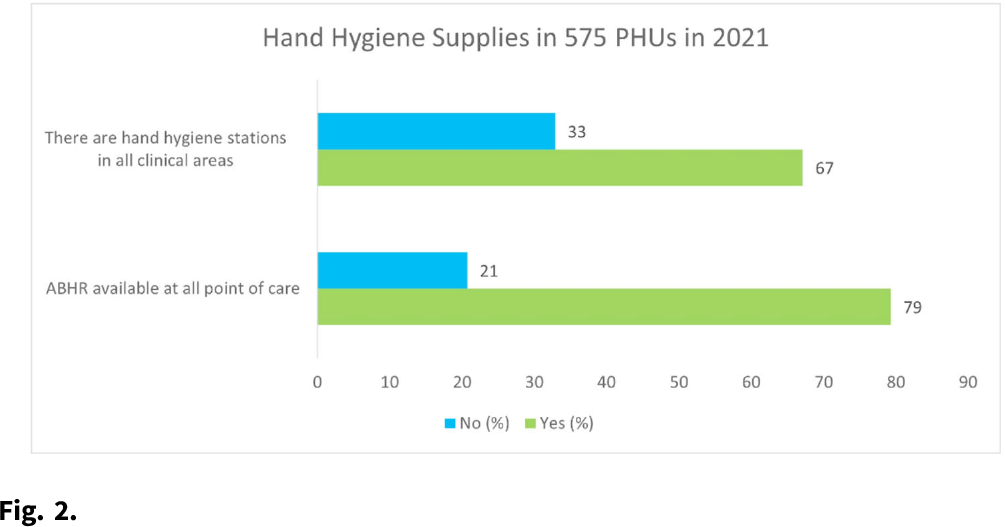
Background: Hand hygiene (HH) remains arguably the most effective way to prevent healthcare-associated infections (HAIs) and ultimately improve the prospect of patient safety. Studies have shown that as many as 50%–70% of infections are transmitted through hands due to poor HH practices. HH with use of alcohol-based hand rub (ABHR) is preferred over handwashing with soap and water because of its wide microbial efficacy, time efficiency, and improved skin tolerance. It is also well known that ABHR can be used as an effective prevention measure during disease outbreaks. Before and during the COVID-19 pandemic, health facilities in Sierra Leone have been challenged with HH infrastructural problems such as lack of sinks with constant running water. Before Sierra Leone recorded its first case of COVID-19 in March 2020, the consumption of ABHR in the health facilities was estimated to be 24,000 L per year, which doubled during the COVID-19 pandemic. The demand for commercially available ABHR increased, leading to acute shortages. The estimated cost of the locally produced ABHR ~$2–3 per 500 mL, although it may cost up to $10 for 500 mL when buying imported ABHR products from the local market. Methods: All ingredients were procured locally, and ABHR production was based on WHO formula 1. The production was set for 12 months to cover the estimated annual consumption of ABHR, with periodic monitoring to ensure effective distribution and availability at the point of care. Analysis of assessment results in 12 hospitals from the pre-COVID-19 era (2019) to the COVID-19 era (2021) was performed based on the WHO IPC Assessment Framework (IPCAF) indicator. Results: With an average monthly production of 3,482 L, a total of 41,780 L ABHR was produced and packaged in branded 500-mL containers for distribution to healthcare facilities. This quantity exceeded the estimated demand for ABHR during the COVID-19 pandemic. The data show a considerable increase (from 25% to 44%) in the number of available and functioning HH stations with mainly locally produced ABHR. Results from the monitoring of 575 peripheral health units (PHUs) in 2021 also showed that >67% of PHUs had HH facilities in all clinical areas and that the locally produced ABHR was used in 79% of these HH stations. Conclusions: Locally produced ABHR has shown to be a cost-effective and evidence-based intervention to optimize HH at the point of care. Therefore, localities are encouraged to undertake this realistic and sustainable approach to address issues of acute shortage of ABHR, especially during a global pandemic.
Funding: None
Disclosures: None


A pilot study of using thermal imaging to assess hand hygiene technique
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s48
-
- Article
-
- You have access
- Open access
- Export citation
-
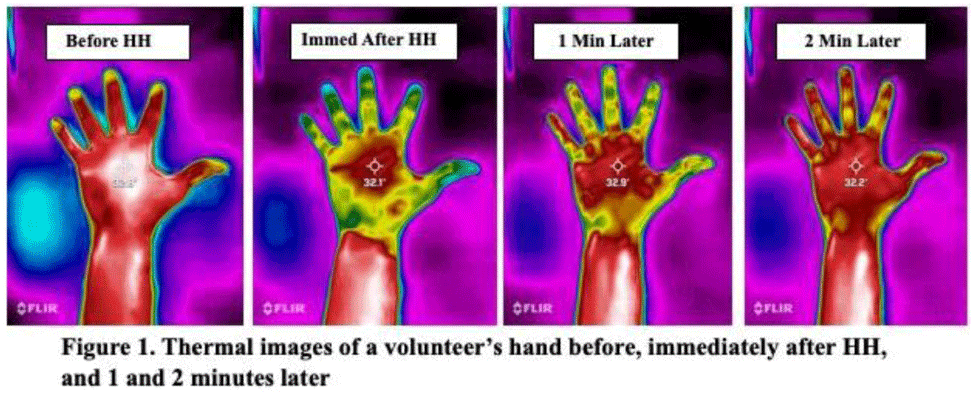
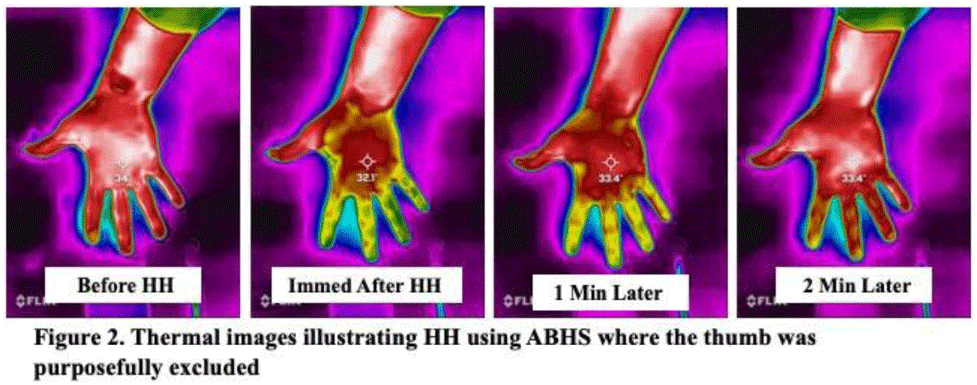
Background: Although substantial efforts have been made to improve hand hygiene (HH) compliance among healthcare personnel (HCP), much less attention has been devoted to improving HH technique. To date, no standard method for assessing HH technique has been widely adopted by hospitals. Because applying an alcohol-based hand sanitizer (ABHS) transiently reduces adjacent skin temperature, we explored the feasibility of using thermal imaging to determine whether ABHS has been applied to fingertips and thumbs, areas often missed by HCP. Methods: A convenience sample of 12 Quality and Safety staff volunteered for the study. A FLIR One Pro thermal camera attached to an iPhone was used to obtain thermal images of the palmar aspect of each volunteer’s dominant hand before applying ~1.8 mL ABHS gel, immediately after hands felt dry, and at 1 minute and 2 minutes later. Spot temperature readings of the mid-palm area and middle finger were recorded at each time point. The sex and estimated hand surface area (HSA in cm2) of each volunteer were recorded. Results: In 11 of 12 volunteers, thermal imaging showed a significant decrease in mid-palm and middle finger skin temperatures after performing HH (paired t test P < .01 for both), especially for the fingers and thumb, indicating that ABHS was applied to these areas (Fig. 1). When HH was performed with ABHS and the thumb was purposefully excluded, the lack of colorimetric change in the thumb was visible (Fig. 2). The palmar area showed the least drop in temperature and reverted to normal temperature more quickly. Immediate post-HH mid-palm temperature change ranged from +0.5 to −2.7°C, with a significantly greater mean temperature drop with small or medium hands than with large hands (Mann-Whitney U test P = .048). With some volunteers, the color changes lasted 1 minute or longer. However, for persons with “cold” fingers at baseline, it was more difficult to draw conclusions from the gross assessment for colorimetric change. Conclusions: Thermal imaging of HH performance shows promise as an HH assessment technique and may be useful to determine whether HCP have applied ABHS to their fingertips and thumbs. Additional studies involving a much larger number of HCP under varying conditions are needed to determine whether thermal imaging can be a practical modality for teaching HH technique, for routinely monitoring HH technique, or as a research tool for studying the dynamics of HH using ABHS.
Funding: None
Disclosures: None


Infection Control in Low- and Middle-Income Countries
Prescribing of common outpatient antibiotics for respiratory infections in adults amid the COVID-19 pandemic in Brazil
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s48-s49
-
- Article
-
- You have access
- Open access
- Export citation
-
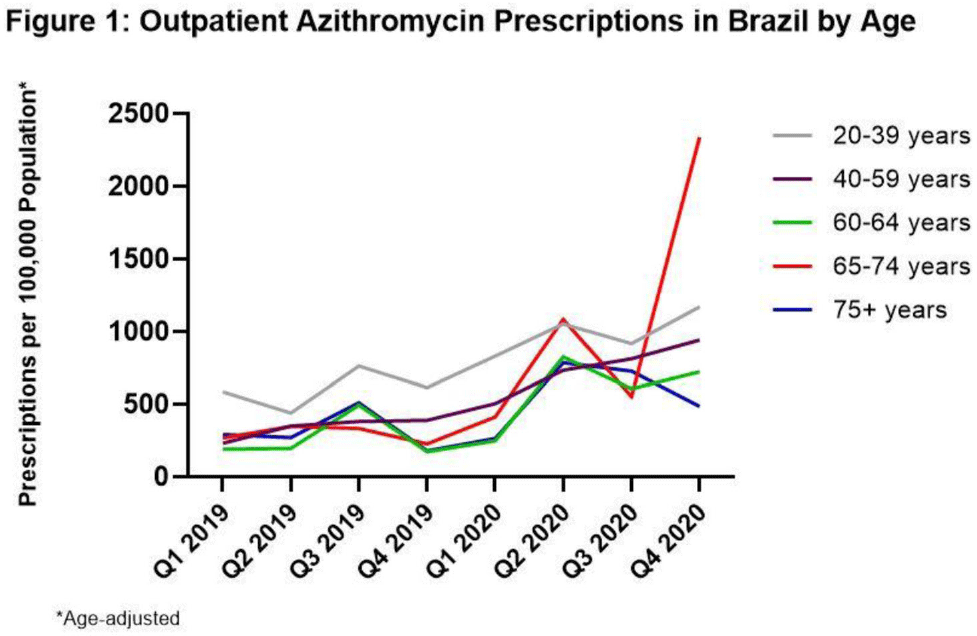
Background: Inappropriate antibiotic use for SARS-CoV-2 infection has the potential to increase the burden of antibiotic resistance. Brazil experienced spread of a new SARS-CoV-2 variant in the fourth quarter (Q4) of 2020, resulting in the highest case counts in Latin America, raising concerns of antibiotic overuse. To better understand antibiotic use during the COVID-19 pandemic, we evaluated prescribing changes in antibiotics commonly used for outpatient respiratory infections (amoxicillin-clavulanate, azithromycin, and levofloxacin or moxifloxacin [AALM]) among adults aged ≥20 years in Brazil in 2020 versus 2019. Methods: We analyzed the IQVIA MIDAS medical data set for AALM prescribing by age group (20–39, 40–59, 60–64, 65–74, ≥75 years), comparing Q4 2020 rates to those in Q4 2019. We estimated crude rate ratios and 95% CIs using prescription number as the numerator (assuming Poisson counts) and age-adjusted population as the denominator. We also determined the most common prescribing specialties for each antibiotic across both time points. Results: Compared to Q4 2019, Q4 2020 azithromycin prescribing increased among all ages, ranging from 90.7% (95% CI, 90.0%–91.4%) in those aged 20–39 years to 927.2% (95% CI, 912.9%–941.7%) in those aged 65–74 years (Fig. 1). Amoxicillin-clavulanate prescribing decreased for most ages, ranging from −78.4% (95% CI, −78.7% to −78.1%) in those aged 60–64 years to −25.8% (95% CI, −26.6% to −25.0%) in those aged 65–74 years. Prescribing of levofloxacin or moxifloxacin decreased for most ages, ranging from −39.1% (95% CI, −39.4% to −38.8%) in those aged 20–39 years to −16.9% (95% CI, −18.1% to −15.7%) in those aged 60–64 years. For those aged ≥75 years, prescribing of amoxicillin-clavulanate and levofloxacin or moxifloxacin increased by 13.2% (95% CI, 11.9%–14.5%) and 43.1% (95% CI, 41.7%–44.5%), respectively. In Q4 2019 and Q4 2020, the 2 most common prescribing specialties for azithromycin were general practice (48%–50% of prescriptions) and gynecology (19%–25%). Compared to Q4 2019, infectious disease specialists in Q4 2020 saw the largest decline in percentage of azithromycin prescriptions (10% to 1%) and surgeons saw the largest increase (0% to 7%). General practitioners were also the most common prescribers of the remaining antibiotics (43%–54%), followed by gynecology for levofloxacin or moxifloxacin (25%–29%) and otolaryngology for amoxicillin-clavulanate (14%–20%). Conclusions: Despite decreases in prescribing of amoxicillin-clavulanate and respiratory fluoroquinolones for most adults, azithromycin prescribing increased dramatically across all adults during the COVID-19 pandemic. Targeting inappropriate outpatient antibiotic use in Brazil, particularly azithromycin prescribing among general practitioners, gynecologists, and surgeons, may be high-yield targets for antibiotic stewardship.
Funding: None
Disclosures: None

Virtual assessments of infection prevention and control practices in African neonatal facilities: A pilot study
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s49
-
- Article
-
- You have access
- Open access
- Export citation
-
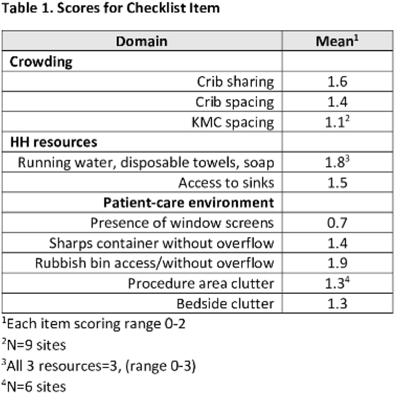
Background: Evidence-based infection prevention and control (IPC) practices to reduce healthcare-associated infections in low- and middle-income countries may be difficult to implement due to lack of resources. We pilot-tested the feasibility of virtual assessments of IPC practices in African facilities caring for small and/or sick neonates for opportunities to improve IPC. Methods: We created a checklist (in English and French) to assess IPC practices in African facilities caring for small and/or sick neonates Results: In total, 10 sites participated in this pilot study. Among them, 3 sites had unreliable Internet connections, and all checklist items could be observed and scored in these videos and photos. The lowest scores occurred for kangaroo mother care (KMC) spacing and presence of screens (Table 1). Conclusions: This pilot study demonstrated the feasibility of using virtual assessments of IPC practices. We identified several potentially low-cost opportunities to improve IPC. We are recruiting additional sites to confirm the findings of this pilot study.
Funding: Bill and Melinda Gates Foundation
Disclosures: None

Disruptions to essential health services in Kenya during the COVID-19 pandemic – February 2020–May 2021
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s49-s50
-
- Article
-
- You have access
- Open access
- Export citation
Long-Term Care
Using a learning needs assessment to develop infection prevention training for certified nursing assistants
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s50
-
- Article
-
- You have access
- Open access
- Export citation
Long-term care facility employee infection prevention adherence and prevention of COVID-19 outbreaks in a high-incidence area
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s50-s51
-
- Article
-
- You have access
- Open access
- Export citation
-
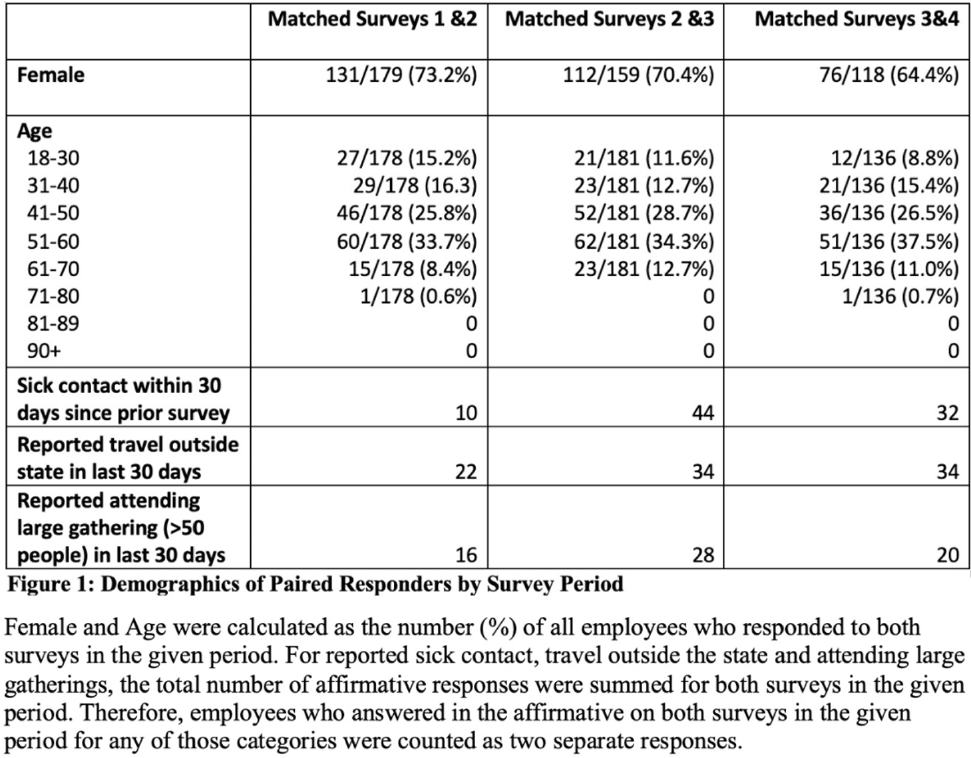
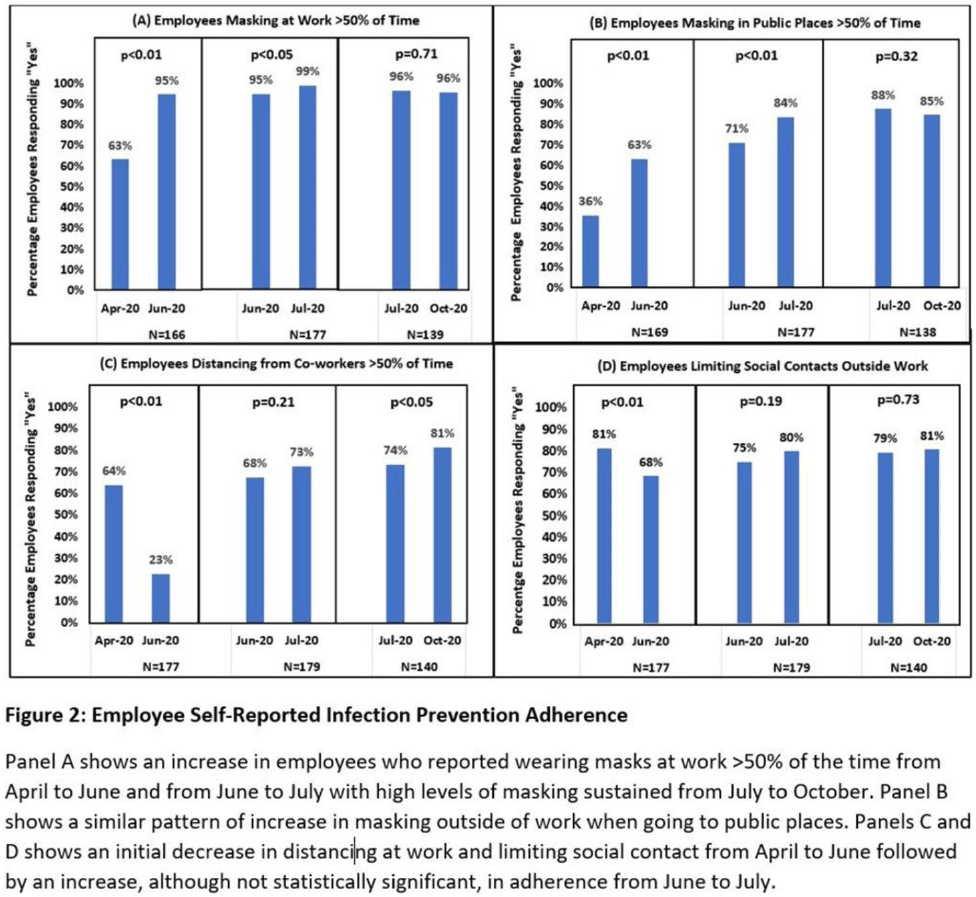
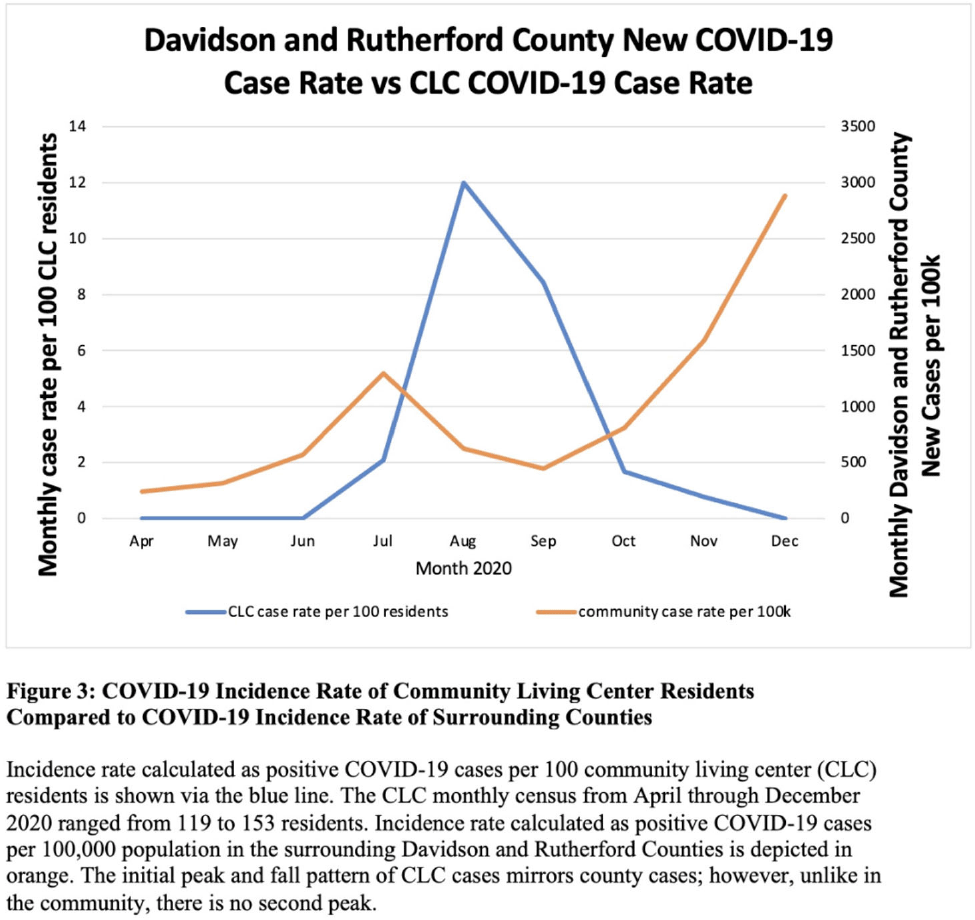
Background: Long-term care facility (LTCF) employees pose potential risk for COVID-19 outbreaks. Association between employee infection prevention (IP) adherence with facility COVID-19 outbreaks remains a knowledge gap. Methods: From April through December 2020, prior to COVID-19 vaccination, we tested asymptomatic Veterans’ Affairs (VA) community living center (CLC) residents twice weekly and employees monthly, which increased to weekly with known exposure, for SARS-CoV-2 via nasopharyngeal PCR. Employees voluntarily completed multiple choice questionnaires assessing self-reported IP adherence at and outside work. Surveys were longitudinally administered in April, June, July, and October 2020. Changes in paired employee responses for each period were analyzed using the McNemar test. We obtained COVID-19 community rates from surrounding Davidson and Rutherford counties from the Tennessee Department of Health public data set. CLC resident COVID-19 cases were obtained from VA IP data. Incidence rate and number of positive tests were calculated. Results: Between April and December 2020, 444 employees completed at least 1 survey; 177 completed surveys in both April and June, 179 completed surveys in both June and July, and 140 completed surveys in both July and October (Fig. 1). Across periods, employee surveys demonstrated an increase in masking at work and outside work between April and June (63% to 95% [P < .01] and 36% to 63% [P < .01], respectively), and June to July (95% to 99% [P < .05] and 71% to 84% [P < .01], respectively) that were both maintained between July and October (Fig. 2). Distancing at work and limiting social contacts outside work significantly decreased from April to June but increased in subsequent periods, although not significantly. COVID-19 community incidence peaked in July and again in December, but CLC resident COVID-19 cases peaked in August, declined, and remained low through December (Fig. 3). Discussion: Wearing a mask at work, which was mandatory, increased, and voluntary employee masking outside work also increased. CLC COVID-19 cases mirrored community increases in July and August; however, community cases increased again later in 2020 while CLC cases remained low. Employees reporting distancing at work and limiting social contacts outside work decreased preceding the initial rise in CLC cases but increased and remained high after July. Conclusions: These data from the pre–COVID-19 vaccination era suggest that widespread, increased support for and emphasis on LTCF IP adherence, especially masking, may have effectively prevented COVID-19 outbreaks in the vulnerable LTCF population.
Funding: None
Disclosures: None



Experiences of nurses responding to the COVID-19 outbreak at a long-term care hospital in Korea: A qualitative study
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s51
-
- Article
-
- You have access
- Open access
- Export citation
MDR GNR
Pseudomonas aeruginosa bacteremia mortality and resistance trends in the Veterans’ Health Administration (VHA) system
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s51-s52
-
- Article
-
- You have access
- Open access
- Export citation
-
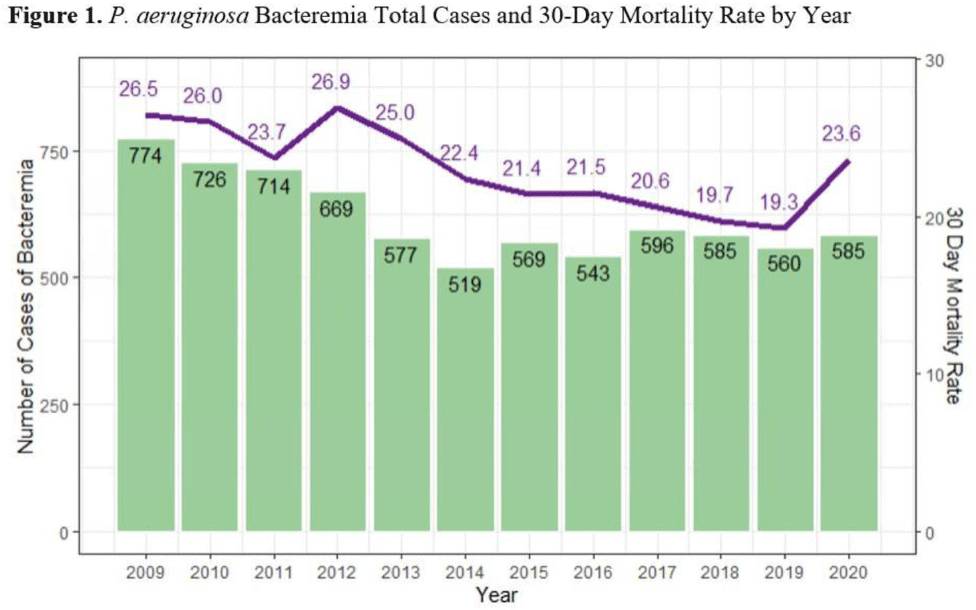
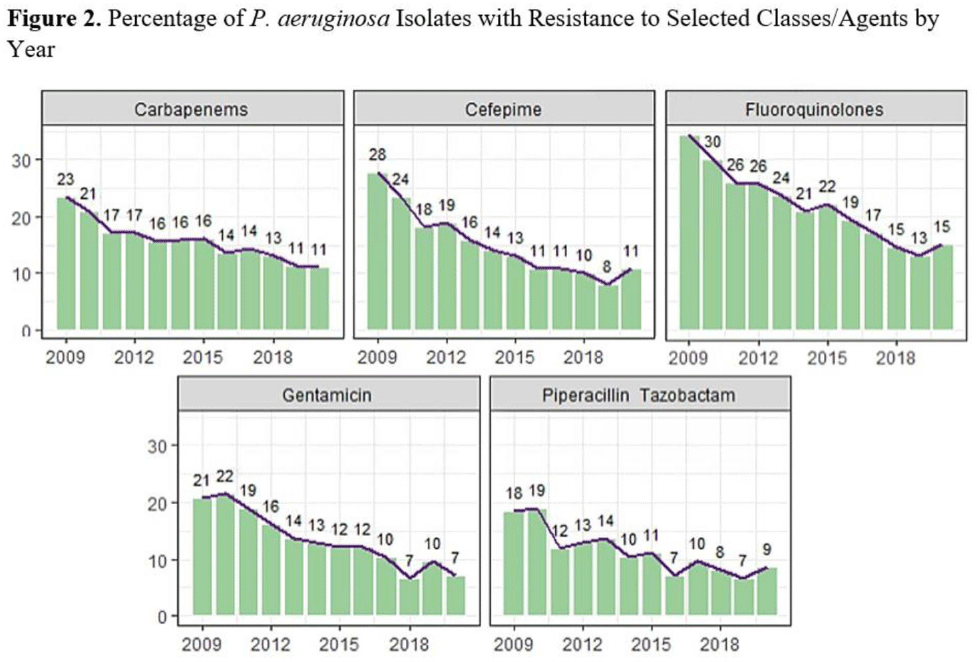
Background:Pseudomonas aeruginosa is an important pathogen in the hospital setting; it has the ability to cause severe disease and a high mortality rate. Its increasing ability to elude even novel antimicrobial mechanisms of action is a significant cause for concern. More effective treatment options and increasing understanding of this pathogen likely effect P. aeruginosa incidence and severity; however, longer-term studies are lacking. The Veterans’ Health Administration (VHA) population is a socially, demographically, and medically distinct entity, representing a rich source of data for studying contributing factors to P. aeruginosa infection and mortality. We sought to identify the system-wide case count and mortality rate of P. aeruginosa bacteremia and the rate of resistance to antipseudomonal agents over the course of several years. We described trends observed over the study period. Methods: We utilized the nationwide VHA database to identify all inpatients with a positive blood culture for P. aeruginosa treated between January 1, 2009, and December 31, 2020. We identified the annual count of bacteremia cases and associated 30-day mortality rate. Additionally, we determined rates of resistance to antipseudomonal agents. Results: In total, 7,480 cases of P. aeruginosa bacteremia were identified. The total case count of P. aeruginosa bacteremia decreased from 774 in 2009 to 519 in 2014, then remained relatively stable. The 30-day mortality rate decreased from 26.5 in 2009 to 19.3 in 2019, but this rate increased to 23.6 in 2020 (Fig. 1). The fluoroquinolone class had the highest resistance rate at 23%, followed by ceftazidime, cefepime, and the carbapenem class with rates of ~15%–16%. All classes were noted to have decreased resistance over time (Fig. 2). Conclusions: Occurrences, mortality rate, and associated resistance of P. aeruginosa bacteremia across the VHA system generally decreased during the study period. Potential explanations for these observations include improved infection control measures, more effective therapeutic agents, and enhanced antimicrobial stewardship efforts. The increased mortality in 2020 could be related to concomitant COVID-19 or the result of delayed medical care in the pandemic setting. Limitations of this study include inability to identify causative factors for observed trends and potential variability between labs affecting the rates of observed resistance. Additionally, VHA data may not be representative of entire adult population. Future studies could explore the relationship between P. aeruginosa bacteremia and infection prevention and antimicrobial stewardship efforts and could describe associations between P. aeruginosa and COVID-19 and identify risk factors associated with P. aeruginosa bacteremia and mortality.
Funding: None
Disclosures: None